IMHO we need more schools and we need better medical schools that produce more dedicated students to the growing problem that ACA (which I believe is a good thing) has created.
It’s a numbers game with ER’s closing in major hospitals due to the increase in non insured patients coming to them for help.
I propose (IMHO) that the federal government get all the way into the health care field by starting an affordable accredited medical school for men and women that want to become doctors, nurses, paramedics, in home care givers etc.
If they can afford a web page for ACA that cost an estimated 3/4 billion dollars then surely they can afford a medical complex that can be a training facility for all of the future medial personnel that will be needed due to baby boomers and ACA alone.
They should make it affordable to the tune of covering the cost with service for X amount of years to the VA and to military hospitals as a way to recoup the cost of such a venture.
Peace Corps medical students are needed overseas too … lots of needs out there.
Now we need a plan that will keep ACA affordable for many years to come.
I would hate to see it go down the drain due to lack of medical personnel.
The government’s going to be struggling to fund the ACA. I don’t think we’re going to see it funding more medical schools (which, by the way, are extremely expensive to operate) or more residency slots (which represent the real bottleneck in medical training, as completing an accredited US residency program is a requirement for licensure).
Is there really a shortage of doctors? There’s a shortage of doctors who want to work in emergency rooms or be general practitioners maybe, but I think we have plenty of doctors, and plenty of schools to produce them. It’s not like very many doctors move off to a different career area after graduating. Some states already have programs to pay tuition for future doctors if they practice the needed fields within the state for a period of years.
This article from July 2013 show an increase from 125 to 141 Medical/Osteopathy programs between 2002 and 2013 with a 30% increase in graduates expected by 2017.
It also points out that there is a serious lack of residencies to support that many new MDs or ODs. The limiting factor has been congressional support for funding of new positions. A proposed increase in residency positions was defeated during the healthcare reform debates.
This has been going on with pharmacy for the past 10 or so years, and now, for the first time in recorded history, we have a glut of them. Most places will only hire new graduates, because they can, and some people are even doing residencies and fellowships, which pay a fraction of a “regular” pharmacist’s salary, just so they will have a job. Some are even working as technicians, with tech pay, for this reason.
Problems are best left to the Free Market: eliminate all government regulation and oversight; permit the owners to charge what they like to students; free up the definitions of ‘medicine’; allow the owners to import immigrants from anywhere they wish to come as students, and you won’t recognize American Medicine in 10 years.
There is such a government medical school. It is called USUHS. Whne I went to medical school it was ranked dead last but the most recent US News ranks it in the 50s. It’s free with the caveat that you give I think 7 years to the military.
Also, many people are not aware that the government basically subsidizes medical education anywhere if you join the military. In that case it’s a year for a year. About 1/3 of my class was military. They got full tuition and a stipend for living and book and in return they gave up several weekends and I think 2 weeks of training a year, had to do a military residency if needed, and did 4 years in the military starting at Captain. You can see why nobody wanted to go to USUHS when they could get almost a free ride anywhere else with less payback time. Also, doing your training at military residencies is not necessarily a bad thing. I voluntarily did a rotation at Walter Reed during my residency, which I thoroughly enjoyed except for the problem of having to get up at insanely early hours.
Just to clarify one tiny point in the OP, Peace Corps volunteers do not generally provide medical care as a doctor or nurse. There are health volunteers, but they focus on public health projects-- things like improving nutrition, organizing (but not personally teaching) midwife training, running HIV-prevention programs, and trying to stop the spread of infectious disease. A volunteer might help out at a well-baby visit, but you aren’t going to be getting direct care from one.
Like others have said, it’s not an overall shortage of doctors, but rather a shortage of doctors in certain fields like primary care, pediatrics, emergency medicine, etc… We have plenty of say… anesthesiologists and radiologists, but not so many GPs these days.
My thought is that maybe the residency rules should be changed for some of these specialties and allow say… primary care physicians to do a residency at a doc-in-a-box type place, or for pediatricians to do their residencies in low income clinics, etc… rather than in-house at a hospital.
That, and the obvious solution of subsidizing the tuition and/or insurance for the specialties that are needed which don’t pay so well relative to the others.
As others have said it is the lack of residencies that is the bigger bottleneck, and the fact that people are avoiding fields like primary care.
Another way to address the shortage is more nurse practitioners and physician’s assistants who can act as primary care providers. If they can’t address something they recommend you to an MD. But I would assume a lot of primary care visits are fairly benign to the point where a NP or PA can address them.
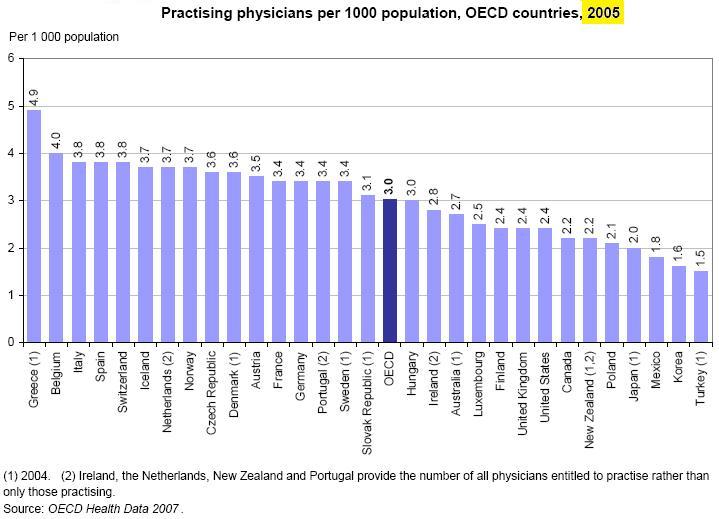
The US has fewer per capita physicians than most other western nations.
I thought there was something like this, but I lacked the details … thank you psychobunny
and everyone else that offered up their thoughtful advice. I didn’t know that about the Peace Corps either some of them I have met in St Croix, VI and they seem like nice enough dedicated people to train to enter the medical field.
We, meaning the USA, have military schools for the Army at West Point and the Navy at Annapolis and the Air Force in Colorado and the Coast Guard in Connecticut.
I think we should start a US Medical school and admit people the way they do at the military academy’s based on desire and grades … not income.
I thought I saw an article somewhere that more doctors are going to be needed when ACA gets it’s footing so to speak. I’ll go look for it
As those articles note, the ACA just amplifies what is already in progress. Hospitals that offer residency training programs have incentives to train more specialists. Lifestyle and income factors push more to specialty medicine as well. An aging boomer cohort that is living longer will require more care and much it primary care. People currently uninsured who become insured are expected to use more primary care as well.
OTOH there is no reason to believe that the medical delivery system cannot adapt; in fact the evolutionary process is already in progress. Physicians are learning how to work better as parts of health care delivery teams and to work with various “extenders” (physcian assistants, nurse practioneers, etc.). The system is learning how to leverage new technologies. Incentive structures are changing such that compensation is not tied to volume but to population outcomes which in turn motivates healthcare delivery systems to figure out better how to provide the best possible care without forcing the patient to come in as often. Electronic communication not just by messaging but in some cases by devices in the patients’ homes that report back weight changes in those monitired for congestive heart failure, daily blood pressures, blood sugars, and a host of other data all of which can be handled and flagged according to algorthms and attended to by medical staff early and sometimes without visits required. Mental health screening and care integrated into the primary care environment (which can significantly reduce medical issue morbidity and utilization). So on. Leveraging the technology is in its early days and the technology avalialable to leverage will become more powerful and cheaper over the next decades.
No question that face to face relationships matter and that the in person physical exam is not going to disappear. But good healthcare teams are becoming more incentivized to create the ways to provide the best care instead of the most care, to compete on the basis of documented value rather than to just see more rooms, and these are fundamental changes that may alter the numbers of physicians needed per capita.
It is an evolutionary process and bluntly put some physician groups won’t survive it. Some models will be tried out and will fail miserably. But I really do believe that result be that we learn how to do this job of providing care to populations as well as the individual better and more efficiently.
I had never heard of this school until I saw your post. Did you ever practice with anyone who graduated from there?
And what is your experience with Caribbean-school graduates? Some did their residencies at the hospital where I used to work, and to me, they were indistinguishable from American-school graduates. Several of them were, based on my dealing with them, some of the best doctors I’ve ever encountered. And then there were a couple that I don’t know how they even got in there, but that was true with some American graduates as well.
The only time I saw a doctor kicked out was probably THE best doctor who passed through that hospital’s residency program, and he torpedoed his career by being arrested for and convicted of domestic violence.
Unfortunately, this underscores the reason that doctors don’t want to go into primary care. The attitude is that “well, a NP or a PA can do whatever a primary care physician can and if the problem is too complicated they can refer them to a real physician (specialist)”. Is it any wonder that nobody wants to go into primary care? Why give up 7 years of your life and thousands of dollars for medical school and residency when you can get an equivalent job with half the training? Unfortunately, the more we rely on auxiliary providers for primary care, the fewer physicians will want to go into primary care.
This is not to say that I don’t value the benefits of a NP or PA. Some of them are much better than many physicians I have known. I have no problem with them caring for my patients, particularly for urgent visits or routine well care. I am just saying that the attitude is demoralizing, living day to day with the pervailing opinion that one is only a primary care physician because they couldn’t hack it as a specialist. (FWIW, I do know my value, which is why I can take care of a lot of problems without having to refer to a specialist and I tend to use the specialists as technicians to do procedures after I diagnose the problem). However, studies have shown that while nurse practitioners order more tests and referrals than physicians, the overall costs are offset by the fact that they spend longer with each patient and therefore charge less money hourly per patient.
All of this is fairly moot, however, because the trend is toward NPs getting doctorates in nursing so that they will legally be able to be called Doctor. Also, the specialists are increasingly using NPs and PAs as physician extenders. You may not realize it, but when you are hospitalized and a cardiology or gastroenterology consult is called, the doctor that sees you is often a doctor of nursing and not of medicine. Again, it all depends on the individual. There is a neurology group around here where I tell the patient to see the NP since she is IMO much better than the physician. However, despite this, nobody is going around saying that NPs and PAs can do the job of a gastroenterologist or a neurologist the way that they do with primary doctors.
As for graduates of USUHS or Caribbean medical schools, the few I have met seem as competent as US trained physicians. Remember, though, that primary care is so undervalued in this country that at many primary-care residency programs the majority of residents are foreign-trained anyway.
Western Michigan University has selected 35 candidates for it’s inaugural class at the brand-new Medical School in Kalamazoo. Good luck to all concerned.