Really. Is that a general nursing thing or something specific to where you work? I’ve never heard of that restriction (not that I’d have any reason to). What about things like morphine (in a hospital setting)?
Really? Are you 12? Some HIV drugs or chemotherepy drugs could do you a great deal of harm. Same with heavey duty cardiac drug.
It’s part of the Nurse Practice Act, but each state has their own. I’d be shocked if any of them didn’t include the requirement that a nurse know the safe dosing, adverse effects and contraindications for each and every drug s/he administers, and refuses to administer any unsafe drug. Failure to do this can get you in front of the nursing board, who will decide the egregiousness of your error and can take action ranging from verbal reprimand to licensure suspension or revocation.
And yes, the 80mg dose is specifically singled out in the 2010 Nursing Spectrum Drug Handbook.
It’s a common book, and it or one like it are available in most hospitals or doctors offices. If the nurse doesn’t know the information about the drug she’s asked to administer, she’s expected to go look it up. Ignorance is not a defense if you give an unsafe medication.
I can give morphine as prescribed as long as I feel that it’s a safe dose. If a doctor accidentally writes a prescription for an unsafe dose (say she writes “10mL IV push” instead of “10mg IV push”) I have to refuse to administer it and clear it up with the doctor before I can give the appropriate dose. It doesn’t matter that the physician made the mistake, I am still responsible for what I do, and that includes not following physician orders if they’re unsafe. We’re not their handmaidens, they are not our superiors, and I can’t get my butt out of a legal sling by saying, “but the prescription said…!”
Is there no packaging at all? Are they in blisters? There might be a code/number imprinted on the foil that would be the drug’s DINif the package is of Canadian origin. You can search the Drug Product database at Health Canada here.
That makes sense. I suppose it’s true that Oxycontin really wasn’t designed for “HOLY CRAP I just broke my elbow” type pain anyways and I doubt it’s doled out in ER type settings anyways.
WRT to morphine I was just curious if you can give that to someone that’s not opioid tolerant if you can’t give Oxycontin to someone who isn’t.
But you brought up another question. If a doc writes an order to do something and you don’t think it’s correct, what’s the protocol? If you go back to him/her to double check and he refuses to change the order for whatever reason, is there something you can do so you can follow the orders but not put your job in jeopardy? I mean, OTOH, what happens if you refuse the orders and something happens to the patient? It’s still your ass on the line, right? Maybe the order was correct or maybe even if it wasn’t correct you needed to get the doc to move that decimal point to where it belongs so the patient can still get the meds they need.
Whoa, “Go Ask Alice (The Goon)” flashback.
True. But there’s also always the risk that pharmacy might send up the wrong med, or the doctor might have a brain fart and write down the wrong thing on the order. I got a doozy once when I was in school: Dr. wrote “Warfarin 100mg PO Daily” instead of “Warfarin 10mg PO Daily”. Warfarin is rat poison, literally. A small dose is given to people to prevent blood clots, but it’s almost always in the 7.5-10mg range. I’ve never met anyone on 100mg of warfarin daily, and if I gave it, it could cause serious, perhaps fatal, internal bleeding
I call her and say, “I want to check this drug order on patient John Doe with the recent onset atrial fib. It says 100mg Warfarin, but that seems unsafe to me. Can you tell me what you meant to order?” Most of the time, that’s all that’s needed to clear things up, because most med errors are just that: errors. A slipped decimal, the wrong unit of measurement, etc. The doctor cancels the incorrect error and tells me the new one. I can give meds on a verbal order, and the doctor has 24 hours to get a written order into the record.
If they yell at me (which sometimes happens) that of COURSE they meant to prescribe 100mg of rat poison, I’ll try again. This time I make sure I repeat the name of the drug several times: “The usual dose is 7.5 to 10mg warfarin. I am not going to give 100mg of warfarin. 100mg of warfarin is not a safe dose. Is there something else you’d like to try?” This is where they often realize they meant a different drug, where the dose would be appropriate. “Warfarin, what? No, no, Wellbutrin!” :smack:
If they still refuse to admit a mistake or change the prescription, then I go to my charge nurse and tell him what’s going on. He can choose to give the medication himself, and then I’m off the hook. (The charge nurse IS my supervisor.) Or he can agree with me and call the doctor for clarification. The charge nurse is the first link in the chain of command. If the charge nurse won’t help me solve the problem, I call the Director of Nursing.
I can give either one to someone who is not opioid tolerant, but in lower doses. A person who’s never had morphine will probably get a 5mg tablet of it (assuming other pain medications aren’t working), while someone in chronic pain who’s been on morphine for a long time may get more than 200mg extended release! Morphine has no concrete upper range, and this is why we HAVE to know your drug history. Honestly, I don’t care if you smoke weed, but if you do narcotics, I need to know that so I can give you enough pain medication to work without giving you so much that you stop breathing.
Back to the OP for a minute: Is it a pill or a capsule? The only thing I can find in any color with a black 40 on it is a capsule: Zerit oral.
It’s a pill, and no, they were free pills in a bag in an old bag, so no blister pack or bottle. I’ll take another look at them and see if there is anything else that might help.
WhyNot, thanks for such an interesting discussion! My sister is a nurse as well (she’s on her way to her Masters right now, such a smarty pants!) and has told me similar stories about dosing mistakes and how she has to handle them. Thanks goodness for nurses! Seriously, they are a patient’s last line of defence and the one that usually gives the best bedside treatment!
There’s a possibility it’s some sort of supplement, either herbal or otherwise. I have a small bottle that I keep ibuprofin in (or whatever) that has some leftover St. John’s Wort pills in it (from my mom; I haven’t thrown them away yet). They’re small, peachy pills (circular, though) with a black STJ printed on them. There’s also just one small yellow pill that’s got 81 printed on it in black type; I don’t know what that one is (but I’m thinking it could be some sort of baby aspirin).
This is precisely why you should carry medication in their original or pharmacy bottles. Sure, it takes up space, but then you avoid this situation (yeah, I know, how often does it really happen? My sister carried her arthritis meds in a ziploc baggie because she couldn’t open the child-proof bottles during bad flare-ups! ;))
Since they were loose, it is possible the imprint on the reverse side may have been rubbed off? Are you sure there’s nothing there? It might help rule some stuff out, though I haven’t really come up with any possibilities. Depending on their age and the type of drug and coating, there’s a chance that the storage conditions resulted in a yellowing of the tablet, so the colour you’re seeing might not be the original one. I’ve only seen that happen in development products under harsh stability conditions, but it’s possible, if not probable.
Actually, I think both of those are low dose aspirin. St. Joseph’s has the STJon it. Here’s the yellow one with 81 on it, also aspirin.
I’ve only seen St. John’s Wort in capsule and tincture (liquid) form.
Snickers - a small yellow tablet with 81 printed on it is most likely to be Aspirin Delayed Release. It’s a common dosage given to maintain heart health for people with cardiac problems, IIRC.
Oddly enough, I’m enjoying this challenge to figure out what these tablets are!
The fact that you say the “40” is printed in black indicates there’s probably some sort of coating on the tablets (when no coating is needed, it’s more common to simply stamp in the ID). Is the tablet shiny like Advil or more powdery looking like regular Tylenol? Is the printing centred on one side, or offset? Is the tablet scored? Is there anything at all that might be a logo of some sort? A triangle, a wedge, a blob?
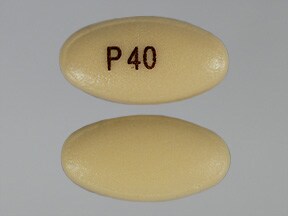
Assuming something may have faded off, pantoprazole sodium delayed release 40 mgcomes closeto your description - does someone in your family have GERD?
{kind=link}
Otherwise I’m thinking they might be some sort of generic ibuprofen (several are stamped with things like IBU 400, which could have faded), dimenhydrinate (gravol) or loperamide (immodium) - common travel drugs.
That’s it, except without the P! That’s exactly what it looks like.
I don’t know if anyone has GERD in the family. Would this be something we would be given in another country for travellers sicknesses or nausea?
The fact that there’s no “P” means it could be something else, though.
I am neither a doctor nor pharmacist and I’m pretty much only going on the information on the link I’ve posted…it seems the only off-label use is for laryngitis. Did anyone lose their voice once while on vacation?
Hm, I did lose my voice about five years ago. I can’t remember a prescription, but I do remember going to the doctor. Maybe it’s from that?
Partly, sort of, solved, I guess!
It’s something a lot of people take *incorrectly *for occasional upset stomach or acid indigestion. Doesn’t do any good, but a lot of people use it. It’s proper use requires a 6 week or so regimen of daily use, and it only really starts to be effective at week 2, and sometimes not until week 8.
Wouldn’t you just be immune to pain for a while? That’s why people love those things right?
No, I’m not 12, and I was actually not serious. Although my guess is that the odds are kinda low that the pills are in any of the categories mentioned.
No, you would also have a depressed heart rate and respiratory drive. Did you not read anything WhyNot wrote about dozing opiates?
No I didn’t. I guess I should huh?