Lots of modern humans migrated out of Africa less than 200 years ago and some are even still there!
After migrating out of Africa many adaptations to other places occurred, but somehow I don’t think intolerance to out-of-season foods (the original point I argued against) is one of them, because that doesn’t seem to convey any benefits so there wouldn’t be any evolutionary pressure towards such an adaptation. If something like this did evolve obviously it would have to be in populations living at higher latitudes which makes it really hard for it to be a universal trait.
If you mean meats that have been preserved with lots of salt and/or nitrates/nitrites, sure. (Those are at least mildly carcinogenic.)
But “processing” is a much-encompassing term, which can range from simple cutting and cooking to whatever the hell it is that MacDonald’s does to chickens to turn them into nuggets. But less than appealing as that may be, I don’t see how such processing is automatically bad for your health.
And what exactly is the problem with sugar? If the amount is within reason and you’re taking in an appropriate amount of calories, the sugar is simply used to fuel your daily bodily processes and activities and that’s that. (The fact that humans and closely related primates can’t synthesize vitamin C shows that we’ve been eating fruit for a long time and are thus used to eating sugars.)
The relationship between alcohol and several cancers (notably breast cancer) seems pretty well-established and is linear IIRC. A little alcohol does seem to protect against arteriosclerosis. I’m not sure if there are any studies that show whether the protective effect on arteries outweighs the additional cancer risk. I don’t drink and I don’t see any reason to start (no family history of cardiovascular disease) but on the other hand someone who drinks a few glasses a week wouldn’t have any reason to stop.
If you do not drink, do not start. Alcohol in moderation is beneficial. In excess it not only can cause cancers, but many other problems too. including brain degeneration, diabetes, cirrhosis, etc.
The first bit is not to defend the point you were disputing but to call out the silliness behind the evolutionary “logic” you used.
“Processed meat” as defined in the medical literature, such as here (that one documenting the increased risk for T2DM and heart disease):
“Added sugar” is also as defined in the actual literature and does not include sugar found in the whole food, like in fruit, but added to the food. The data at this point is pretty rock solid that too much added sugar increases the risk of obesity, diabetes and heart disease. “Much” in this case means much over 100 calories from added sugar a day for women, and 150 for men, which comes to 6 tsp for women and 9 tsp for men (most Americans take in 2 to 4 times that much).
And to be more specific, the annual flooding of the Nile, the tropical monsoon climates, the chilly highlands, South Africa’s Mediterranean climate…seasons are pretty fundamental to a lot of African life.
The link for the full article doesn’t work for me, but I’m pretty sure that study shows correlation, not causation. Obviously people who are overweight or obese are more likely to use added sugar, that extra weight has to come from somewhere.
I don’t see any fundamental reason why more than 25 or 37.5 grams of sugar would be problematic, but I guess in practice it’s true. If you’re trying to reduce your daily calories then having a secondary delivery system for them (drinking) is not exactly helpful. As for solid foods with added sugar, if you like that stuff it’s hard to resist, and if you don’t like it why are you eating more than 37.5 grams worth of sugar?
(I allow myself 5 cookies (60 grams) for desert, containing 20 grams of sugar. I did have to find cookies that taste good enough to be satisfying but not so great that I can’t limit myself to 5.)
It was actually a 2010 review … for a study, here’s a recent one.
Yes, nutrition data rarely randomizes people into long term double blind placebo controlled treatment arms. They do however control for known confounders, in this case including exercise levels, BMI, and educational attainment. The hidden confounder is always possible, so maybe 99% and not 100% … Oh, it is also consistent with a host of animal models, such as this one that shows that added sugar increases liver damage in a high fat diet with a sedentary lifestyle. Also other animal models demonstrating dyslipidemia, insulin resistance, and so on, from much added sugar intake.
And while BMI was controlled for, the argument against too much added sugar holds even if the mechanism of harm is the fact that added sugar hits the centers of the brain that tell people to eat more without hitting the parts of the brain that say that’s enough calories already, and thereby contribute to obesity. Duh yes that stuff is hard to resist … your last comment hits one (but clearly not the only) aspect on the head: foods with much added sugar are not generally very satisfying and have taste good enough that without those satiety centers getting rung the palatability/hedonic center keeps you going.
Oh. A few other comments … that seasonal dietary changes bit … how did you read that as intolerance to out of season foods? The question, and it is an interesting one, is wondering if seasonal variation is diet (both content and quantity) had any particular impact on health that is now no longer as present. I have no idea what the answer is but it ties into the “thrifty gene” concept. The idea there is that populations who lived with significant seasonality and decreased food supplies (especially of foods with adequate fat and carbohydrate) for a few months of the year (which included many populations that experienced winters) would have a benefit to storing fat efficiently during other times of the year, an impact that would constrained by the nature of the foodstuffs and lifestyle in more ancient times (high fiber, moderately high protein, regular physical activity) but that which taken out of that milieu and placed in the context of the modern diet and inactivity is very maladaptive.
Also your bit on “… you can either have bad habits or be overweight, but both of them will land you an early grave” - most studies end up showing that both have some impact but indeed even the “don’t be obese” one is not quite 100%. Some argue that the impact is not the obesity itself but correlation of obesity with poor cardiorespiratory fitness (CRF); see for example this meta-analysis.
100% is hard to hit. Stating that there are strong correlations of certain complete dietary patterns and fitness levels with longevity and quality of life lived … that is simple. Proving which of the items is a key item independent of the others … not so simple.
Its not that simple. If you are feeling stressed, worn out ,sore, sick, depressed it probably helps to improve your diet… Of course you should also try to avoid emotional situations, get some sun , some relaxation (at least half an hour power walk a day, or a few hours if you can … but just the half hour of sun) …
That is kind of amazing. You’d expect the lowest category to do especially good because that’s the one with all the health freaks that only eat raw walnut shells, but the risk increases progressively with more sugar intake.
Unfortunately, that still doesn’t tell us whether reducing your sugar (and not making any other changes) confers any benefits. Maybe cardiovascular disease makes people develop a sweet tooth rather than the other way around. But considering the limitations on human experimentation this is pretty much as conclusive as it gets, so I’ll make an effort to move down a quintile or two in my sugar consumption. (Good thing the days that I took my tea with a tablespoon of sugar are long gone.)
Hm, then people living at higher latitudes would have to be more prone to obesity than ones historically living closer to the equator, and that doesn’t seem to be the case. For instance, Polynesians seem quite prone to obesity and Northern Europeans not more than average.
It’s also possible to argue that if food availability goes up and down throughout the year then populations would have adapted not just to storing fat when food is abundant, but also to shedding fat when food is scarce, rather than just keep accumulating fat.
Now I wonder how fit I am…
But the good news is that we can tell people: “don’t be fat, do be fit” so even if they can’t maintain weight loss at least they can be fit and avoid disease.
One of the issues is that we’re now three or four steps removed from actual disease. I.e., if someone has a blocked coronary artery, the artery is stented or bypassed, so the disease is treated directly. But we know that arteriosclerosis is promoted by bad cholesterol levels, so now we check for those (1 step removed) and then give people statins to lower their bad cholesterol (2 steps removed). And tell people with no cholesterol problems to avoid eating foods high in cholesterol such as egg yolks to avoid getting bad cholesterol to avoid arteriosclerosis to avoid clogged arteries to avoid a heart attack. Obviously somewhere in this game of telephone the message can get lost.
We know exactly how people get fat: eat more calories than the body uses. If you don’t do that, you don’t get fat, save for a fraction of a percent of the population with certain endocrine disorders.
Cancer on the other hand, is a crapshoot. Yes, some games pay out more than others, but even a fair number of people who do everything right get cancer.
No, it is very direct. You add in a few steps. I don’t care what the mechanism is. Eat one of a wide variety of sorts of diet (all of which are not the typical Western industrial food fare and which typically include lots of fiber rich foods, as a marker) and stay physically active and the odds of you living longer and living better the years you live go up significantly.
BTW, in terms of Polynesians … there we are dealing with whence the founding population came from and founder effects. While I am not sure what I think of the hypothesis that observation does not falsify it.
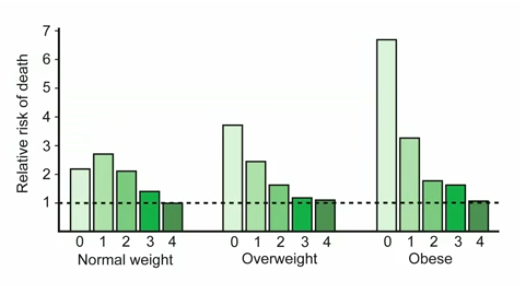
The fourth factor was moderate alcohol consumption which means 1-2 drinks a day. The death rate among the overweight matched thin controls after one healthy habit was added, among the obese it took two. I don’t know the name of the study but the Ted talk was from Sandra aamodt
I agree with point 1 and 2, but don’t know what order 3-5 would go (is diet better than oral hygiene, is exercise better than diet, etc). I’ve heard about the connection between poor oral hygiene and inflammation, which can trigger system wide inflammation. Ten years ago people laughed at me when I brought this up in polite conversation. People are assholes. What were we talking about again? Oh yeah, lifespan.
other lifestyle factors that are important to lifespan and health span are:
Strong, meaningful social connections
Low stress/good stress control
Good quality sleep
Meaningful work and hobbies (I believe this is an independent factor)
Here is the chart from Sandra aamodt. For whatever reason (I don’t get it) thin people who have 1 healthy habit have a higher death rate than someone who has 0, and a thin person with 2 has the same death rate as someone with 0. That seems fishy to me. Someone who is thin but who also smokes and never exercises should have a higher death rate than someone who doens’t smoke and does exercise.
As far as overweight & obese, it takes 1 (of the 4 lifestyle factors) to reduce death rates among the overweight to that of thin people and 2 for obese people.
There was a big study several years ago finding overweight people had a lower death rate (possibly due to extra lean body mass, I’m not sure the mechanism). So I’m confused why the death rate would be higher among the overweight vs the thin, shouldn’t it be lower?
I find the counting of the habits counterintuitive…
One factor could be that the among the people who have all unhealthy habits / lack all healthy ones the death rate the ones most sensitive to the risks have already died to a notable degree so the remaining ones tend to be more immune than average against unhealthy habits.
As for the protective effect of being overweight, one criticism is that the normal weight category also includes people who are suffering from diseases like AIDS and cancer, so the effect isn’t actually real.
Smoking and exercising both reduce weight, so the overweight group probably has more people who don’t smoke but do exercise, who would be relatively healthy, and people who do smoke and not exercise, who would be relatively unhealthy. I’m pretty sure eating or not eating a banana once in a while isn’t going to make up for that.
I’ve heard that criticism, but I do not know if it is proven or just a hypothesis about the lower mortality rate among the overweight. FWIW, various issues like being a minority, being poor, or using various drugs for medical conditions (SSRIs, antipsychotics, corticosteroids, etc) can cause fat gain or are associated with a higher BMI, so the same argument could be made in reverse. How much of the health risk of being obese is just because poor non-whites with health conditions are more likely to be obese?
I don’t know if exercise alone really reduces weight in a meaningful way. I’m trying to find some studies I’ve seen in the past, but I recall reading people who live in urban areas and do a lot of biking/walking only weigh a few pounds less than people who drive.
Y’know, these last few posts have done a wonderful job of illustrating just why we don’t have 100% rock hard information about human longevity. It’s really hard to pin down exactly what is responsible for what.