Depends on the particular circumstances, I’d assume. Just how much hepatic dysfunction there is, whether they were actually encephalopathic or not, how habituated they were to the opioid, how good their renal function was (as an alternate pathway for drug metabolism), etc. So basically a clinical, bedside decision to be made.
I sure would not want to be messing with additional mixed opioid agonist/antagonist drugs, who knows what sort of effect one would end up potentiating/blocking in those situations.
Otherwise, drug holidays are good ideas, along with keeping in mind that the goal of the opioid use for chronic, nonmalignant pain is to improve function, not to relieve pain. It’s chasing after pain relief that causes a lot of the problems. Target specific objective functional goals that are currently not achievable due to pain, see if those goals can be safely met with judicious use of the opioid; if not, stop using the opioid.
Despite being a doctor, your own issues with opioids might be coloring your viewpoint. People with debilitating pain sometimes cannot lead normal lives without some form of relief. I used to suffer terrible migraines. Opioids did nothing for them. Conversely I’ve also had excruciating back pain off and on for years that only opioids could relieve.
I’m 64 and have been on and off of opioids since my 20s. They can work for long term pain without negative effects. Yes, it’s a huge pain in the ass to come off of them during the periods of heavier use but if that’s the price to pay for being able to function, so be it. And at it’s worse it’s better than being bedridden AND being in pain.
Pain drugs cause legitimate problems for many people but to ignore the debilitating aspect of pain that some people suffer and say “opioids are bad, take Tylenol” is a very Pollyanna way address their issues.
True that and you’d have to be in their shoes to know pain. Without injections and pain pills I’ll put a bullet in my head. That’s how bad it is.
I found another way to treat pain, it’s called drinking. It’s better than the crap pain pills they pushing on us.
Well, but that Rx is extremely toxic to the liver as well.
Except that peer reviewed studies have shown the Doctor to be correct.
As time goes on the pain relief provided by the opioids gets smaller and smaller and the addiction gets stronger and stronger. Some peoples claim of pain relief is actually the addiction getting a hit.
So of course you could be exceptional, but in general, opioids don’t provide significant pain relief after years.
I am actually one of the few docs out there who think the pendulum has swung too far, away from proper use of opioids. During the heyday of the whole horrible “pain is the 5th vital sign so prescribe opioids until the patient is free of pain because people in pain don’t get addicted or abuse drugs” debacle, I posted online here and elsewhere how I thought that was a bad idea and would lead to overprescribing and all sorts of unintended consequences, and suggested we focus on function, not pain, as the thing that needs improving in our patients’ lives. And that people with a history of substance abuse should not be considered for opioid therapy for chronic non-malignant pain save as an absolute last resort for only very specific situations. And even for folks without a history of abuse, opioids are still the 5th or 6th or 7th option to consider for management of their chronic situation, certainly not the 1st or 2nd. (Not my original ideas, this was propounded by other, wiser docs before me and I just agreed loudly)
That got ignored of course, until too many died of opioid overdoses for us to ignore anymore, and now things are far more draconian regarding the prescribing of opioids than I ever proposed. It’s a huge PITA to write for the stuff now, which I have to do regularly, as I have hospice patients under my care too.
But opioids for chronic use are the wrong choice for well over 90% of people with chronic pain issues. And I will stick by that, based on the best objective evidence I’ve seen.
However, I acknowledge that still leaves some thousands of folks who can safely benefit from them. Finding out which those ones are, and treating them with opioids is a much harder challenge than it used to be (not that it was ever easy). But keeping opioids out of the hands of the other 90+% of patients will save many lives, so we need to do this.
Yeah but Rx opiates aren’t whats killing people, it is chinese fentanyl that is killing people.
Pain destroys quality of life and productivity. There need to be some effective treatments. I suppose one good thing to come from the war on opioids is that it’ll lead to more investment into alternative ways to control pain.
Plenty of folks od’ed to death on standard prescription opioid pain killers too. Methadone is quite notorious for causing fatal overdoses. I stopped prescribing methadone for pain as a result of that, long before the designer fentanyls became big. Street chemists making sufenta and carfenta, etc just raised the death rates.
Looks like my Lupin (made in India) pain pills does have hydrocodone in them but the test doesn’t show how much there is. I got relief from Watson and Actavis but not with the Indian crap (mallinkrodt and Lupin).
According to this, death rates from synthetic opiates have skyrocketed. Natural & semi-synthetic opioids seem to make up 1/3 of the growth in deaths, but the deaths from synthetics have skyrocketed since 2013.
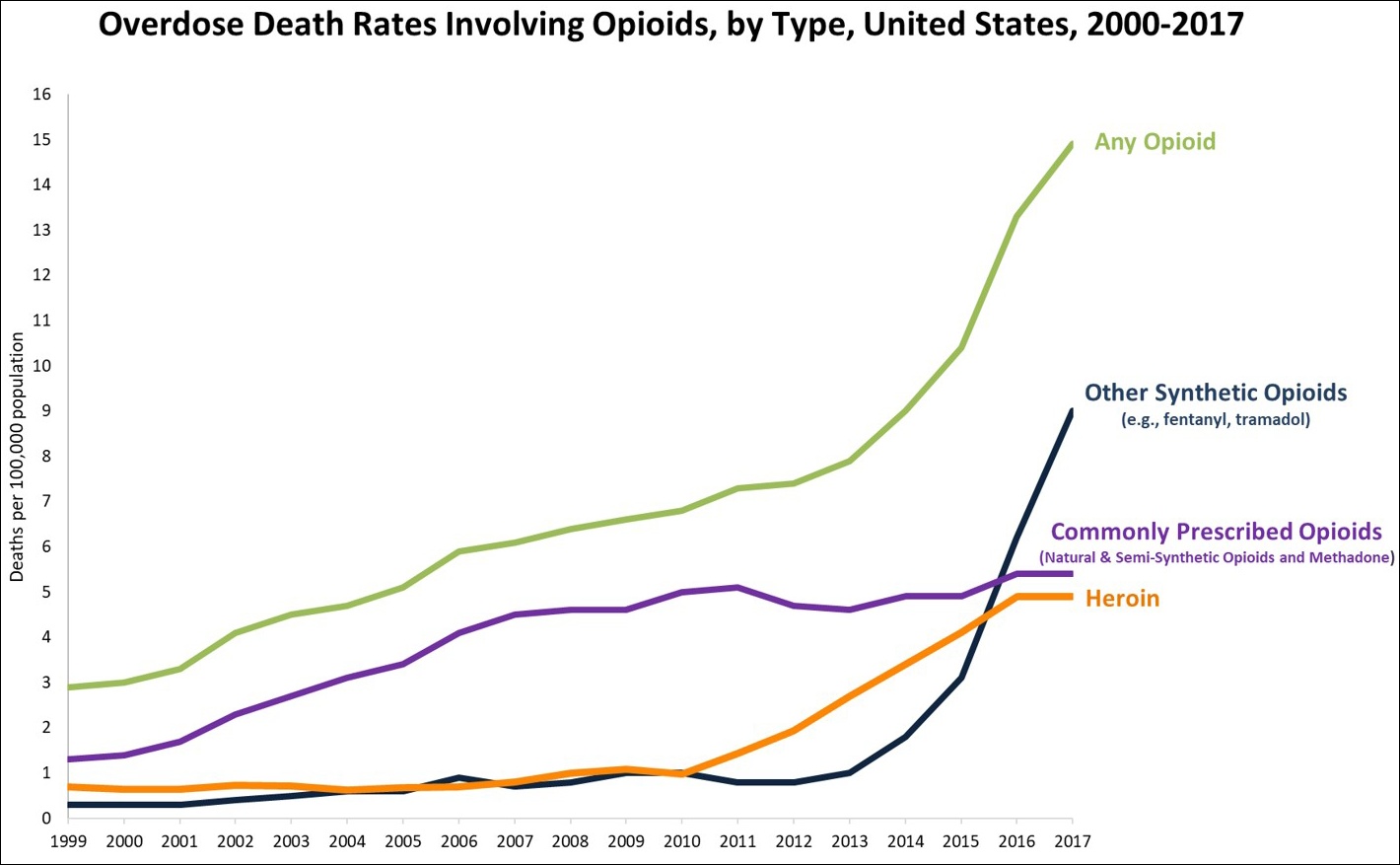
I’m confused as to why heroin death rates went up so much. I’m not sure if that is because they are cut with synthetics or if there is some other reason.
I think it’s because of the potency. It wasn’t cut as much it used to.
I’m one such person. Ive been on an opiate for over 10 years without increasing my dosage. I don’t know that there is anything ‘different’ about me, maybe it’s about what i expect out of the medication?
You’re one of those very fortunate people who has found the exact drug and dosage that works for you. ![]()
I have a friend who has had lap band surgery, and severe arthritis in her knees and hips due to her former obese state. (or, at least, the one hip she was born with) She has figured out how much hydrocodone she needs to keep severe pain at bay, and that’s all she takes. Since she had the more severely affected hip replaced, she has been taking much less, and then only for her knees, and by now not even every day. She does not get any kind of buzz from it, or pleasure beyond the pain relief.
I guess I’m one too. I’ve been taking 5/500 since 91 but take injections for trigger points which is my neck and lower back. The pills alone won’t be enough to control pain. I noticed that when they reduced it to 5/325 it wasn’t that effective as it used to.
My guess is that my relief came from APAP as well as Hydrocodone. Few months ago I told my doc that I’m not getting relief like I used to so he gave me 7.5/325 since then. It wasn’t any better hardly.
Now the Indian crap they’re handing out are worthless.
Tramadol has been around for years as a treatment for chronic pain. It’s an opioid analgesic that doesn’t get most people high, and I think the people who do say it makes them high are the same people who buy black market Prozac to get “high.” It does make some people feel tired, even sleepy, but typically not what anyone would call an opiate-like high. It is prescribed for mild to moderate pain.
I’ve taken tramadol for post-op pain, and it has a certain distinct opioid euphoric effect on me, just dialed waaaaay down compared to oxycodone or dilaudid, etc. I’ve seen a lot of recovering opioid addicts take it because it was first presented as ‘non-addicting’, and end up abusing it, and/or moving back to other opioids. Other recovering addicts have used it successfully (in that they took it as prescribed, stopped when it was no longer needed, and didn’t relapse to other opioids). It should be used with great caution by folks with a history of addiction.
If I may ask a related question: Has someone tried small doses of ketamine to reduce pain? Does its nature require that pain reduction must be accompanied by loss of lucidity?
Do dissociatives have an “opposite” drug like stimulants vs depressants that could counter some of the negative effects of ketamine?
It’s a NMDA antagonist, so anything that acts as an NMDA agonist is roughly opposite. Glutamate is the main ligand agonist. The problem is that NMDA receptors are so prevalent and drugs differ both in what receptors they activate and which subsets in the body they activate so you probably won’t find a true “opposite.”
NMDA antagonists are used as anesthetics. PCP was invented as an anesthetic, and ketamine is used in animals for that purpose.
ketamine is sometimes used in compounded creams for topical application to treat nerve pain (along with other things like gabapentin, lidocaine, etc).
So yeah, they are. However I’m not sure how good the NMDA antagonists are at analgesia because if used systematically the cognitive side effects can be pretty severe.
Some of the cognitive effects of dissociatives can be counterbalanced with antipsychotics. I think at least. I think that’s what they give people high on PCP in the ER.