I’ll try to log on and provide some more data about the US’s out-of-control spending and gross overuse of procedures later. It’s been a wicked long week in the clinical analytics trenches.
I actually meant both articles read back-to-back; that’s a powerful way to read them.
Gawande has also written books. Check them out! (Why, yes, I’m a fangirl…I’ve idly considered moving my medical care from Lahey to Brigham and Womens Hospital where he practices on the off-chance of running into him. THAT is a fangirl! :))
I’m assuming insurance would cover it. If a hip replacement cost $60,000 in the US but cost $10,000 in India, Mexico, Thaliand, etc. or $20,000 in Europe or Canada I’m guessing the insurance company would pay for airfare, hotel, and all medical costs.
A physician in India has managed to cut the cost of open heart surgery down to $1,600 (he still manages to turn a profit at those prices). He wants to cut it further down to $800. in the US it costs $20,000-100,000 for the surgery.
A lot of times, the wasteful treatment or test is required by the insurance company. For example, taking an x-ray of a sinus infection doesn’t demonstrate anything beyond what a regular exam does. Wasteful. If a physician is contemplating surgery, s/he will order a CT to take a look at the lay of the land and so on, which is reasonable. Some insurance companies demand the less-expensive test (x-ray) before the most-expensive test (CT).
I should have been less flip and stated that the majority of the time, out-of-country surgeries and treatments are not covered by US insurance companies.
up_the_junction: The news report you linked doesn’t differentiate between inpatient medical surgeries that would be covered in the US (such as joint replacement) and non-covered surgeries (cosmetic) and those that might or might not be covered by an insurer (gastric bypass).
Coverage by insurance companies for out-of-country surgeries is still available only in ***very ***specific circumstances/treatments/surgeries and for ***very ***specific insurance companies and hospital programs. You can’t just decide that it’ll be cheaper to get a new hip in Australia and jump on a plane.
The majority of policies I’ve seen lately still have out-of-country exclusions.
There are also concerns with liability, HIPAA, any need for recovery time, and illnesses not found in the US when you go overseas (which vary based on where you go).
And the CDC cautions about problems medical tourists may face overseas that they would be less likely to see in the US:
And, of course, there are liability and post-op care issues to consider. If you get a raging post-op infection in your new knee, do you have to get back on the plane? What if the new knee joint is recalled? Do you have to go back?
I’m kind of with Flyer on this one. Medical science has advanced a lot in the last century. We should expect the proportion of the economy going to health care to increase as new categories of treatment and new specialties become widely available.
And–costs aside–the total amount of health care services provided should, if anything, be going up, if PPACA has lowered barriers to health insurance and lowered the share of health care monies that can be diverted to insurer profits.
I’ve worked in health insurance for over twenty years and currently work in healthcare analytics. So yes, I know a little more than the average asshat who quotes a badly-written, badly-researched puff piece.
Technology is not the whole issue, and medical tourism can’t fix everything. U.S. residents pay multiples more than people in the rest of the world pay for even the most basic medical procedures and generic drugs.
One small example: I got ringworm a year ago. It’s a minor fungal skin infection. The antifungal ointment used to treat it, which is on the WHO’s list of basic medications, cost less than $20 in most of the world. U.S. cost for the generic? Almost $300. Ringworm is diagnosed by looking at it: no fancy tests required.
Medical tourism can’t fix everything. Who’s going to be able to move to a foreign country for months or years on end for cancer treatment, for example?
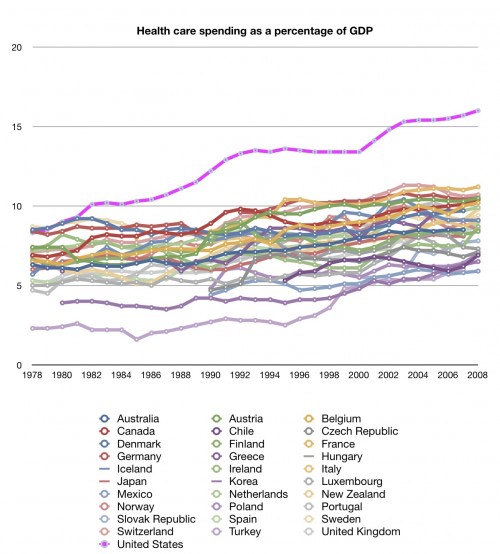
OK, so can we talk about this in a way that distinguishes between a) total health care expenditure as a share of headline GDP and b) actual inflation / price gouging per service rendered?
It might be interesting to talk about the “acute” shortage of nurses (as mentioned in my link above) - given the cost of health care you’d be forgiven nurses weren’t all driving home to their swanky downtown apartments in new German convertibles. Regarding the OP: No one got back to me on my earlier maths point (not my best subject) that, if 8 million people suddenly get on board before costs decrease, of course the percentage of GDP will increase?
Back when I worked at Blue Cross Blue Shield I was involved with the unit that was investigating how to allow “medical tourism” coverage. The cost savings were enormous not just to the patient but to the insurance company back 20 years ago, I’m sure they’re more so today. Yes, there is a risk of oddball infections but you have that here (with a different list of oddball stuff). Doctors in many other countries are just as competent and innovative as American ones. Back before I was laid off in 2007 quite a few BCBS companies were allowing it under defined rules and we can expect to see that trend increase.
So yeah, there are issues with US insurance coverage on medical tourism, but they’re surmountable and it is happening. I fail to see why you dismiss it, and GrumpyBunny, out of hand.
Medical costs follow power law distributions. 1% consume 20-25% of all medical spending. 5% consume 50-60%, 20% consume 80%, 50% consume 97%
Flip the numbers around and you find that 95% of the country uses less than half of all medical spending, 80% use 20%, 50% use 3%. I’m going to assume many who got added via obamacare are relatively low cost patients, so the costs wouldn’t increase much. Most truly sick are on Medicaid, Medicare or some other program already.