These companies have literally thousands of metrics - considering that they span multi-year time periods (as was the case here) - which could be tossed at them. There’s no way they can have all that in their heads at the time they testify. Congresspeople get to cherry-pick the ones that supposedly make their case and toss them out at the “witness” who will inevitably have a hard time responding, no matter who is on their staff.
The consequences of getting it wrong are absolutely zero. As indicated by this thread (and any number of comparable discussions of various blogs and such). Here she tossed out a number which seems to be blatantly contradicted by documented and verified information, and it does appear not make any dent to the adoring crowds, who just accept what she says on pure faith, and her status as “national treasure” to her ideological compadres is only enhanced. She - and others like her - have every incentive to make the most sensational charges in hearings such as this, with little regard for their accuracy.
The Corporate Social Responsibility (CSR) trend may be the start of the systemic change you’re talking about. It doesn’t change businesses’ priorities from profitability to improving society, but aligns profitability with improving society. IOW, customers vote with their wallets against corporations who are seen as egregious polluters, abusers of human rights, etc. Shareholders notice that stuff.
When I worked for an e-commerce company, our products had a price, and they also had a “compare to” price, telling the savvy and sophisticated consumer what they could ‘expect’ to pay for a similar product elsewhere.
That “compare to” number was, of course, pulled out of our asses.
Nobody pays a hotel’s rack rate. I’m not entirely sure why they even exist (but tended to be on a card on the back of each room’s door).
Can Big Pharma deduct discounts from these putative ‘list prices ?’ Are they just used as a starting point from which they know they’ll have to negotiate discounts – that starting point being artificially high in order to settle at something they can live with ?
I found an articleabout proposed legislation that seemed to get asymptotic to this issue, but … honestly … I’m not into it this morning.
I just wonder if there is any economic correlation between the actual COGS on a drug and the “list price,” or if it’s more like our “compare to” or “rack rate” contrivances.
The specific, overall metrics they would need to have are quite obvious. And there’s no inherent reason that they would need to have things memorized: you can have notes.
This sort of hearing on falls over backwards to allow the company to dispute any claims made about them. To act like they’re the victim is ridiculous.
The reason we believe her is the same reason that a jury would believe the prosecution if the defense does not counter their claims. The point of situations like this is to create an adversarial system where both sides will do their best to debunk the other, until the truth is found.
And both are, as far as I understand, put under penalty of perjury. As such, if some evidence is not brought up that logically should have been, the default assumption is that said evidence is known to be inaccurate.
R&D costs vs. advertising costs is something that’s obviously going to be brought up in this type of hearing. If their chosen representative is not prepared to debunk inaccurate statistics, they have only themselves to blame.
I’ll just point out that I do Business Development in the pharmaceutical industry. I’m expected to bring in the best deals, at the greatest profit, and my performance is evaluated on that. I’m at the executive level, and routinely meet with the board. Most of us acknowledge, 'round the water cooler, that the business is out of control. WE see the need for regulation, but the idea that I can personally change the rules of the game is silly. I suppose the board could (we are privately held), but they only care about the money.
Many of us who actually run the company really do care about bringing novel drugs to market, for the good of patients. But we’re paid to make as much money as we can.
I can. But I don’t set pricing. I negotiate agreements to further develop products, license them in, manufacture them, etc. But if I decided to start advocating for better pricing, lower salaries, etc. I’d simply be replaced.
I don’t think what I do is evil. Indeed, I can personally point to life-saving products I’ve helped bring to market. But at the end of the day, the owners get what they want. I’d love to see limits on what we can charge for products.
I’m really glad you spoke up, because I feel I am in much the same situation as you.
I detest the money-grubbing grift health care system we currently have, yet I earn money from a business that would be fully eliminated as pointless (and rightfully so) should this country ever get serious about providing real access to affordable health care for its citizens.
I’m self-employed as a third party administrator of Flex plans and HRAs. I specialize in working with small employers. These IRS-sponsored plans enable both employers and their employees to enjoy genuine and significant tax relief, some of the little to which we hoi polloi still have access. I am glad to help with that.
But should we ever create a true health care system here, my work would be eliminated overnight.
I’m fine with that. I had hoped to be out of business long before now.
My brother works in Financial Services. Has for 30 years. Worked for the same company for 20 years and was a consistently top performer in terms of bringing in assets under management. Was also a top performer in fees generated in dollars, but not in fees as a percent of assets. That is because he would put clients into appropriate (to them) investments, not ones that generated the highest fees and commissions. For the last ten years he was hounded by the management of the company for not maximizing the potential yield of his clients assets. He finally quit and moved to a different firm. Almost all of his “book” followed him. But he is having pretty much the same issues at the new firm already.
Right. And even most of the board members aren’t the Big Money. They are placed there by the Big Money, though a couple are actually Big Money. Shit rolls downhill. And again, I like what I do. I think it has value. And most people would do exactly what the board does, if they too were Big Money. I’ve no problem with making a profit, even a very good profit. But the government, its rules, its purchasing power should stand in balance to the inherent human greed.
Enter the battle for/against requiring all investment advisers to be, legally, fiduciaries:
I won’t claim omniscience on this one, but on its face … you’d think that having
… a duty to act in the best interests of another party. In the case of a financial advisor, an advisor acting in a fiduciary capacity has an obligation to put the interests of their client first when giving advice, as well as in all aspects of the client-advisor relationship.
Would be kind of a no-brainer, no ?
Same old story
Same old song and dance
/
Meet the new boss
Same as the old boss
I hope he continues to be successful, that his business grows because of ethics, retention, and word-of-mouth, and that the myopic bean counters in his world (they’re everywhere) come to understand that LTV (Lifetime Value) is still bankable money.
Meanwhile, I hope he can make peace with the inherent tension between genuinely trying to act like a fiduciary and the Economic Pressures From On High.
ETA: I can’t tell if this one links back to @Mighty_Mouse 's most recent post, so …
Are we sure we’re comparing like and like? The 10-K is for AbbVie and subsidiaries; I can’t find a figure on AbbVie itself, but the company has dozens if not hundreds of subsidiaries around the globe, some wholly-owned and some not.
There’s also a fun note re: that $10.3B: “In 2019, following the announcement of the decision to
terminate the rovalpituzumab tesirine (Rova-T) R&D program, the company recorded an impairment
charge of $1.0 billion which represented the remaining value of the IPR&D acquired as part of the
2016 Stemcentrx acquisition. This termination was subsequent to the decision to stop enrollment for
the TAHOE trial, which resulted in an impairment charge of $5.1 billion in 2018. These impairment
charges were recorded to R&D expense in the consolidated statements of earnings in 2019 and
2018.” (p. 80) In other words, nearly half of that $10.3B was an “impairment charge” as they wrote down the value of a failed acquisition. Are impairment charges really best categorized as R&D expenses?
It varies according to the drug. You may remember the Epi-Pen scandal just a couple years ago. COGS < $1 per dose, list price $600. Pharmacy benefit managers then negotiate down as the manufacturer wants their drug on the formulary, and PBMs (negotiating for insurers) don’t want to pay more than they have to. Manufacturers will have programs for people who can’t afford the drug, eg: self pay or sucky commercial plans. They are prohibited by law from cost assistance to govt insurance beneficiaries as that is essentially cheating the govt into paying 100% when the govt wants the patient to share cost.
Then again some newer drugs involve cloning hamster cells (eg: the Jimmy Carter drug, Keytruda) and other future tech. Probably not enough to justify the list price, but actual expenses aren’t cheap either. Actually come to think of it, that particular kind of manufacturing probably scales very well… but I’m sure there are significant royalties to pay just to use new manufacturing processes.
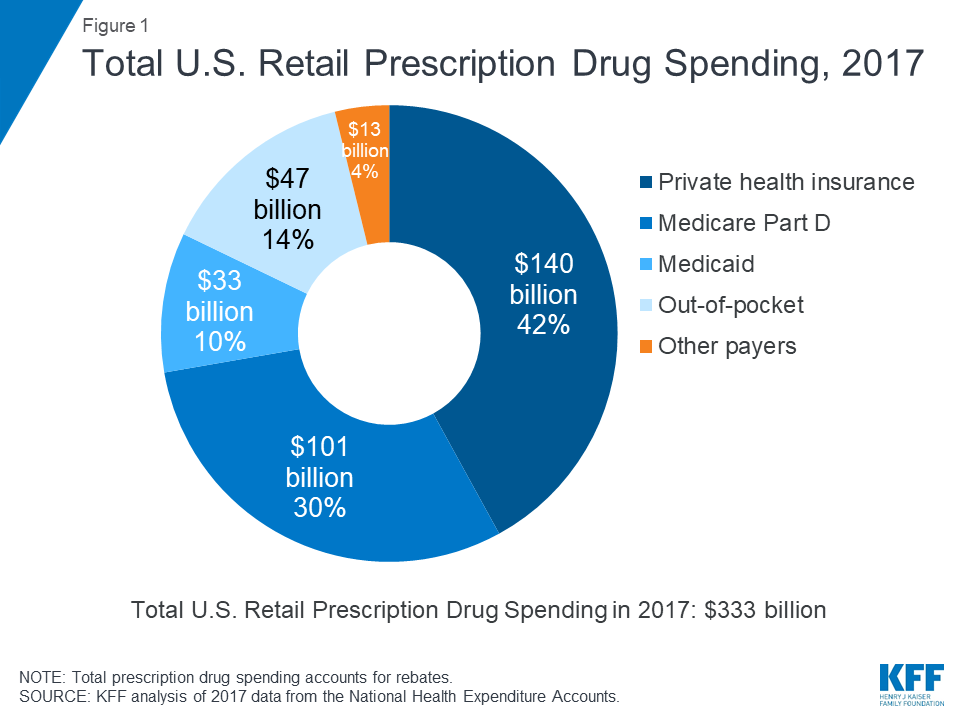
It looks like Medicare pays for about 30% of the drugs prescribed in the US:
And … last I knew … the US was barred from negotiating drug prices with the manufacturers (source).
If most (all ?) Part D policies are administered by private insurers, are they still bound by that “no-negotiate” law ?
What I’m getting at here is: could one reason why drugs like Humira carry a sticker price of $72,000/yr be that the one payor who actually pays full sticker (and who pays for 30% of the drugs in the US every year) is [wait for it] the US taxpayer via Medicare ?
It looks like the government is considered to be an interloper (between the drug companies and the Part D coverage carriers) in this pas de deux, and the government is barred from ‘interfering’ in these price negotiations.
Into how many pieces is that 30% pie divided ? How much bargaining power are we losing in this transaction ?
I may dive into this a bit deeper in the near future, but if anybody has any expertise on it, I’d love to hear your thoughts.
Part D plans are left to negotiate prices themselves. In practice the insurers pool their bargaining power: maybe four out of five Part D plans rely on just three regional pharmacy benefit managers, basically people who specialize in negotiating prices and formulary access (Express Scripts, OptumRx/UHC, or CVS/Caremark).
With respect to any prescription drug, there is no direct relationship between the price agreed upon by the private insurer administering the Part D plan and what the federal government actually pays.
My understanding is that Part D federal expenditures come in the form of monthly subsidies to private insurers. Every year each insurance company submits a bid to the government that estimates total prescription drug expenses for each beneficiary, then they go off and negotiate rates, process and pay out claims, etc. The government takes a national average of these bids each year to get your average prescription drug expense per beneficiary. Each month the government pays approximately 75% of that average to each insurer, adjusted for risk (the insurer’s track record of keeping at/under their bid). At the end of the year the government reconciles the average bid with actual expenses to share gains and losses with the private insurers who administer the plans.
And so? They are not a non-profit company, they answer to their shareholders, the FTC and the SEC.
Why shouldn’t they spend $334 million on Executive compensation?
I have no idea why this is some big deal of investigative reporting, when all that is in their Annual report, available to any stockholder or even the public.
Because they are profiting obscenely on the illness of our citizens, who are paying more for their health care than anywhere else in the world.
There are lots of ways companies can profit. This oughtn’t be one of them. Governments can subsidize R&D, and I suspect it would cost a whole lot less than the truly breathtaking profits realized by drug companies now.
At some point, I’d like to see responsible corporate citizenship should kick in. I’d like a baby unicorn, too.