If Obamacare resembles the private tier of the German system, why are costs so much higher in Obamacare in comparison.
No, reality doesn’t say different. Obamacare was going to reduce average premiums by thousands, but it didn’t.
Regards,
Shodan
If Obamacare resembles the private tier of the German system, why are costs so much higher in Obamacare in comparison.
No, reality doesn’t say different. Obamacare was going to reduce average premiums by thousands, but it didn’t.
Regards,
Shodan
Why the past tense - is it a two year deal or something?
Because the German system authorizes local authorities to negotiate for lower prices: https://en.wikipedia.org/wiki/Healthcare_in_Germany
Either you didn’t read what I wrote in #71 or you completely failed to understand it.
YOU claimed (not I) that “Obamacare is rather similar to the German system”. You made that claim in #62. I spent a fair amount of time explaining in the above-linked post why Obamacare is not anything even remotely like the statutory public system in Germany that 90% of the population uses. That’s why it can’t control costs.
Either you didn’t read what I wrote in #71 or you completely failed to understand it.
This was in reference to your other claim that universal health care in general won’t reduce costs. I explained why, if and when it is ever implemented in the US, in the same manner and with the same regulatory structure as found in the rest of the world, it will, just as it does in the rest of the world.
That’s an important part of it, but not all of it. Very significant cost savings also come from the unified model of common rates and services and true universal coverage. Both of those things are so fundamentally, philosophically different from the mercenary market-driven insurance system in the US that it’s hard to even make comparisons.
Apologies - I didn’t see your post as I kind of stopped following this thread. In any case, looking back, that was not my claim. This was my specific claim:
This was your response:
Of course it depends on how you measure it, but here’s one article that talks about what countries have lead the world in medical research and innovation in the past 20 years.
Then, if you look at medical device patents and country of origin, you come up with about 70% ish originate from the US. (Table A1-2a) Breakout By Country of Origin. I stopped looking at this point, but I’m guessig the same type of lopsidedness in pharmeceutical development would also be true - let me know what you find.
So unless you measure research and development some other way, the US is the world leader and it’s not even close.
You go on to say this:
I’m not quite sure how these statements are relevant or the point you’re trying to make. Medcial spending in the US is huge. Is that the gist?
I don’t think this is true. Cite?
I don’t see how you can reconcile this last statement with the previously quoted section. Europe can’t spend more on biomedical research while at the same time the entire planet’s biomedical research budget is 1/5 of that of the US.
I don’t think it’s relevant that the US government is the largest contributer to US medical research even if I accept this as true, which I’m doubtful of. I think this is onl true if you include and exclude specific things that wouldn’t make sense as a whole. How are you coming to this conclusion? What is relevant, is the potential rewards of the US system. The lure of unlimited payouts for successful research is probably a great motivator. This doesn’t exist if the government is able to exert monopolistic demands on prices.
In any event, I tend to think the US system is crappy. I’m just not convinced other systems as presented are preferrable. I used to think that market solutions for health care were the answer, but I’ve moved away from that as I don’t think the health care market behaves like markets for other types of goods.
To me though, it is unquestionable that the US is the leader in research, development, and innovation. That’s nothing to sneeze at and is not often addressed when it comes to modeling some future system after another country who is not the leader in this regard.
Earlier I asked you how on earth you believed that private health insurance contributed to medical research. You said you meant something quite different and you’ve now clarified it. Let’s follow this logic.
There are many reasons that US health care is so absurdly expensive, all of them directly attributable to the system of private insurance. ONE of those reasons is the inability to control provider costs. So what you’re saying is, a system that is so exorbitantly wasteful in so many different ways, including unlimited profiteering by health care providers, is actually a good thing because it might encourage someone, somewhere, to maybe invest a bit more in medical R&D? Do you realize how ridiculous this is, on so many levels?
Just for starters, a great deal of medical advancement comes from better understanding of disease and treatments that comes from basic medical research, not from companies building better widgets. And most of this research is funded by the federal government. I’m too lazy to go looking up numbers right now but the fact is that the vast majority of all university research is federally funded, and institutions like the National Institutes of Health have enormous federal budgets. Years ago, in fact, one of my academic colleagues here in Canada, a well-known medical researcher, was actually getting more grant money from the NIH than from the Canadian government. The US is just a big, wealthy place with a lot of research money, and a lot of it is rightfully going into medical research, and it has nothing at all to do with the health care system.
Other advancements come from pharmaceutical research, which is a different domain not directly related to provider cost control (Canada, for instance, has some nominal federal laws against pharmaceutical profiteering, and none at all on the cost of generics, while the whole issue of health care cost control is handled at the provincial level and has nothing to do with drugs at all).
And even in the one narrow area of medical equipment, your argument doesn’t hold. So you’re saying that better MRI machines will be developed because a manufacturer can sell 5,000 of them instead of 3,000 of them? Even if that were true – which I very much doubt – is having an absurdly out-of-control price structure for health care that is driving it to the verge of unaffordability the most efficient way to fund that? Really? How much of those extortionate health care costs, if any, actually goes to that R&D? 1%? How about the government controls health care costs, and provide that 1% for equipment R&D? Anyway, I seem to recall that a great deal of top-end medical imaging equipment comes from European manufacturers like Siemens, so even that last vestige of argument doesn’t seem to hold water. Most such manufacturers sell to world markets.
Thank you. The recognition that the free market – which works so well in making and marketing televisions and washing machines and making them available based on ability to pay – doesn’t work at all for health care is the first step in addressing the problem. The next step is for conservatives to come to a pragmatic realization about what does work. I don’t think it’s much of a stretch to say that what works in the rest of the world, even if you don’t accept other aspects of their ideology, will also work in the US if implemented in similar ways.
The biggest hurdle to overcome is that on issues like the ACA conservatives automatically yowl about “government interference” in their health insurance, and what they need to understand is that the thing that they’re yowling about is, in fact, the solution. Close government involvement and oversight is absolutely key to making health insurance workable and universal. In some places governments run the health insurance system, in others they just tightly regulate it. Nowhere else in the world do insurance companies run wild as they do in the US, even post-ACA. With all due credit to Obama for having improved the situation a bit, but those who think that the ACA has brought health insurers in line should reflect on how closely they were involved with drafting it.
Whenever you have to paraphrase you should really question whether you’ve accurately captured the message you’re trying to paraphrase. Starting out with *“So what you’re saying is…” * should be warning bells for you. My original post about the positive utility of US based research, development, and innovation was to introduce this topic as part of the calculus when determining an overall approach to health care. Often these facets of health care are not addressed when doing world wide comparisons. In these regards, the US is the worldwide leader, hands down. While you may think this a ridiculous allocation of resources, it is the current reality. You think this is a bad thing. I’m not convinced.
Those potential ridiculous profits are what drives innovation.
I’m not sure what point you’re trying to make here. Are you not including pharmaceutical research in the mosaic of health care?
I don’t know if it’s the most efficient. What I know is that the vast majority of medical device patents have US origin. That isn’t cherry piking MRI machines, it’s everything. That’s the reality. Unless a proposal addresses this imbalance, why it may exist, and how it will be impacted by proposed drastic changes to the US markets, then I think the analysis is not as persuasive.
You take this idea too far. Just because health care doesn’t behave like typical markets for goods in all cases, doesn’t mean that it doesn’t behave like typical markets in some cases, or that market forces implicit in a given system have beneficial value. I’m not sure what will work, but some element of the market is probably worthwhile.
Except that I think I paraphrased it quite accurately. We agree that there are virtually no effective cost controls in the US health care system. You yourself used the phrase “the lure of unlimited payouts” as being the Great Motivator. What did I get wrong?
Moreover, you keep claiming that “the US is the worldwide leader, hands down”. Whether this is true or not (as pointed out by others, a great deal of medical research takes place outside the US), it’s also true (as I pointed out) that a great deal of it is due to government funding of basic research in a large and wealthy country and has absolutely nothing to do with the nature of the health insurance system. And even if it did – and it doesn’t – that would be an absurdly inefficient way to fund innovation.
ISTM that saying “those potential ridiculous profits are what drives innovation” is just a high-level ideological mantra that in this particular case is just completely factually misguided.
I’m making the point that pharmaceutical research is a big contributor to health care innovation, and yet in Canada, there is no price control over it at all at the level of provincial health care funding, and a minimal amount at the federal level. At the federal level, essentially drug companies are asked to justify their prices for new patent drugs, like why a patient should be paying $10,000 a month for medication. Yet, some drugs do cost that much, because apparently they did justify it. And all of this is in the land of price-controlled universal health care – where, incidentally, a great deal of pharma research goes on.
So??? Some years ago my mother’s cardiologist here in our socialist health care system in Canada recommended that she should have a pacemaker. I was curious about the technology so did some investigating. It turned out to be one of the best models from Medtronic, purchased I’m sure at some exorbitant cost from Medtronic Canada, and followed up later with followup testing by a clinician and a Medtronic technician using what looked like a roomful of test equipment. So guess what? Single-payer and UHC systems buy lots of medical equipment because they need it, they spend a lot of money on it, and they don’t seem to be averse to buying the best. And don’t tell me that the companies aren’t profiting.
I agree. I think that a regulated but competitive kind of free market has a place in the health care provider system. It just has absolutely no place in the health insurance system. Free markets do not have a place in determining who gets medically necessary health care and who does not, and who lives or dies. That’s why health insurance as the sole means of paying for medically necessary, life-saving health care is, at its core, a criminal racket.
But, as I said, it does have a place in the provider system. Again to take an example from single-payer in Canada, I should be able to – and I do – have a choice of any doctor or hospital I want; doctors and clinics are all in private practice, and hospitals, while almost all non-profit, are nevertheless competing for funding on the basis of reputation and patient count. Americans convinced that Canada is running “socialized health care” might be surprised to see Canadian hospitals running lavish websites that are essentially competitive advertising (example 1, and example 2) and doing “patient satisfaction surveys”. The only difference from south of the border: all these places are free for all citizens. Maybe there should be a motto for single-payer: “You choose, the government pays”. ![]()
No. Here is your paraphrase:
If you think this is a fair characterization of my statements then I’ll be glad to no longer respond to you. You let me know what you think.
Again - not sure where you think I agree with this. Your skills at paraphrasing are lacking.
I cited upthread. US is the leader in medical research citations, cross citations with other countries, medical device patents, spending on R&D. I don’t care if it’s inefficient in this context - that’s not the point I’m making. I’m saying, that is reality. The question you need to answer is not whether this is efficient, it’s what the impact to this would be in some future proposed system.
I’m not sure how you reconcile these bolded statements. And, yay Canada. The US is still the leader in pharmaceutical research and development.
In the US, I can no longer get a plan that doesn’t meet the ACA standards, even if a provider wants to supply it and I want to pay for it. That’s a limit on choice.
I’m not sure drones would bring much more to already-existing forms of telemedicine (even going back to the days of WT and Flying Doctors, as in Australia).
First off, you’ve replied to me, but then quoted someone else’s question.
Secondly, thanks for your figures, as they do show you’re wrong.
The US, population of 318 million, has 7.3 million citable research paper. Just looking at the UK, France, Germany, Italy and Spain (317 million people) and you’re looking at 7.1 million citable research papers. Using your metric of citable research papers, all it takes is 5 UHC countries to match the US. Then think about Canada, Australia, Netherlands,Switzerland, Sweden…
In short, for far less money than the US spends, UHC countries are outstripping you for research. Your own link makes this very same point quite clearly:
“Four small European countries lead the ranking of Nobel prizes for medicine per capita, matching their identification with powerful health and pharmaceutical industries. They are in this order Denmark, Switzerland, Sweden — very close together — and Austria further behind. However, new entrants such as India, China and Israel are becoming world powerhouses in the drug industry. It is likely that these nations’ manufacturing capability should induce the innovation drive required to promote them to the top tier in the discipline:”
I get the sense that’s not it’s portrayed on the US Nightly News. I don’t know but imagine, US wonder discoveries come along most weeks. Non-US, not so much.
I thought it might be interesting to offer an idea of the level of scrutiny costs come under in the NHS system - in some ways the data here is extraordinary. Of course, the value of it is to identify where next to attack costs and increase value, which itself often leads to innovation:
Factually speaking, the obscene quantities money spent directly on insurance funded care or drug company sales is not going towards R&D. Almost all the R&D you are talking about is done by various universities, some of whom include teaching hospitals and medical schools.
It is true that private drug companies conduct their own research, however :
1. For economic reasons they have little reason to try for new treatments to life threatening diseases. Better to make a variant on an already known to be profitable drug. This is similar to how the entertainment industry likes to invest it’s money into sequels.
2. Much of the privately funded research by drug companies is suspect and contains a clear statistical bias. (that is, evidence is overwhelming that on average, the research is biased and often wrong)
3. Almost none of the actual money paid by consumers for the overpriced pharmaceutical drugs goes to useful research. The vast majority goes to marketing, profits, and useless research.
You’re right. My mistake.
I wasn’t making a per capita argument - merely gross figures. From the first line of the article:
Which is pointless. Comparing the US (population 320 million) to a country 1/5 it’s size (the UK) will obviously see more papers coming from the US. Do a like for like comparison (as I did) based on a similar population size of 1st world countries, and it is clear the US is not innovating any more than the rest of the world.
But the others are doing it without fleecing their citizens exorbitant amounts for health care.
“merely gross figures”. LOL. Here, let me hold the door open for you >>>>
Your quotes do not, in general support your statement. You are comparing the R&D in a country of 320 million people to countries of 1/5 the population or less. Adjusted for population, the US does not seem to be producing more than other countries.
Patents are not a good measure of research activity unless you do a lot of work adjusting for how patent laws differ from country to country. Genetics patents for example. I also remember from my own days in uni, it was assumed that we would come up with a few patents on our own, and the lecturers mentioned that it was far easier to patent something in Europe tha the US, because the US patent laws gave so much narrower protection. You’d need to spend abut £ 5000 on a patent in the UK, (early 90s) in the US we were warned, you’d need about 30 times as many patents for the same level of protection. Pocket change for a company, prohibitive for an individual.
Now, as I said, I would not be surprised to find that the US dominated medical research for a period after WW2. Only developed country with an intact economy and infrastructure after all. But on a somewhat larger timescale, I struggle to find any of the truly groundbreaking medical inventions originating in the US. A lot of refinements sure. But if you look at the big medical breakthroughs… blood groups and transfusions, anaestesia, antibiotics, X-rays, organ transplants, germ theory of disease, genetics, vaccination, DNA, etc…not US research.
Not quite. Medical spending in the US is so huge that the entire worlds biomedical research spending is dwarfed by the waste in US medical spending. It is therefore unlikly that the US system is in any way responsible for US research successes as US research is simply too small a fraction of the spending.
You could well be right. I seem unable to find my own original cite. I did find this, which seem very detailed, gets quoted a lot, and in general agrees, except the total sum and the Europe sums are lower.
Note, however, that a larger fraction of Europes research is from private sources than in the US.
The entire planets biomedical research budget is 1/5 of the waste in the US healthcare system. US biomedical research (public and private) is 1/10th or less of the waste in the US healthcare system.
I am not coming to a conclusion, I am stating a rather well-known fact. Please google the NIH. This is fairly fundamental.
I would also say it is relevant that Europes systems produce a larger fraction of private spending that the US system.
This seems to be very much at odds with how things actually work.
it seems that similar to other areas of health care, the US spends a lot of money. But does not come up with a lot of breakthroughs. If I were to hazard a hypothesis, I would say that people who are in it for the massive profits are less likly to do good science and big breakthroughs than the ones who are in it for the science.
The way heathcare behaves in markets have in fact been looked at.
It is a discipline of economics called “health care economics” The discipline originated with Kenneth Arrows work on uncertainties in markets, work for which he later recieved the Nobel prize. His seminal work, which gave rise to health care economy, is available online.
Ironically, he is American, and the discipline of Health Care Economics could be said to be the one unquestionable American breakthrough in health care research.
I don’t understand why you’re in a huff as I thought we were having a productive and perfectly civil discussion. OK, you don’t like my paraphrasing, so let’s not quibble about how accurately it reflects what you were saying and just go with your exact words, which were these (in #105): “What is relevant, is the potential rewards of the US system. The lure of unlimited payouts for successful research is probably a great motivator. This doesn’t exist if the government is able to exert monopolistic demands on prices.” And this (in #107): “Those potential ridiculous profits are what drives innovation.”
I and other posters have explained why this is completely unsubstantiated, and the basic reasons can be summed up as follows:
[ul]
[li]Much of the most important health care research is supported by government funding[/li][/ul]
[ul]
[li]The high costs of health care in the US are well understood by health care economists and have nothing to do with anything that promotes health care innovation; they are due to the staggering complexity of myriad private systems operating on the basis of risk-based underwriting as a business, creating a vast cascading series of cost issues which both requires providers to charge exorbitant fees and makes it difficult or impossible to control them. This doesn’t help anyone get better medical equipment or provide better treatment.[/li][/ul]
[ul]
[li]The health care market is relatively inelastic; it’s primarily just driven by the need for health care, nothing else, and such potential profits as may drive private, non-governmental R&D are based primarily on the size of the market. Moreover, such markets are typically global, not just national.[/li][/ul]
[ul]
[li]Far from growing the market, the current system actually works to reduce the size of the health care market, by excluding some 40 million uninsured, and by discouraging utilization through such tactics as co-pay requirements. For example, Canadians visit doctors more frequently and have longer average hospital stays than their US counterparts.[/li][/ul]
[ul]
[li]Looking at gross numbers for research spending as you’ve been doing instead of per-capita or on a GDP basis completely misrepresents the argument, since a major reason US health research numbers are big is that the population and economy are big. Plus, the US is also, in general, a major center of general high-tech innovation for a long list of reasons that have absolutely nothing to do with health care.[/li][/ul]
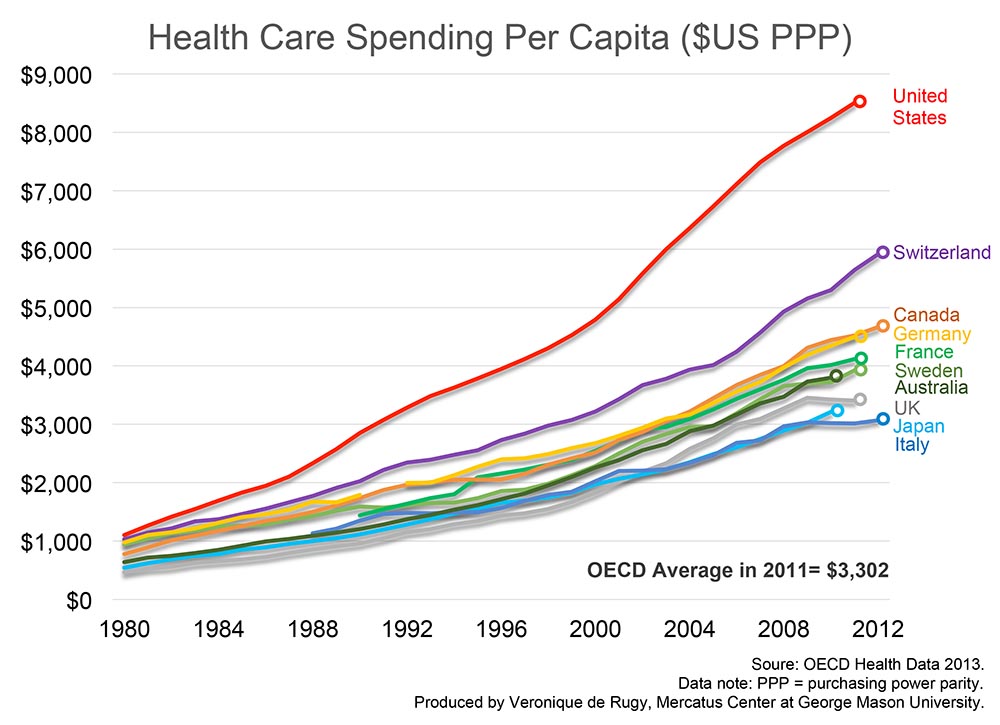
OK. Again, let’s forget the paraphrasing. You say you don’t agree that there are virtually no effective cost controls in the US health care system. Do I have that right? Or if I don’t have it right, perhaps you’d care to clearly tell us just what your beliefs are in that respect so there’s no possible basis for misunderstanding. The basic facts aren’t complicated. Looking at a chart like this, one sees that US costs – and US costs alone among all nations – are literally off the chart; cost charts have to be scaled to accommodate them or else the US graph would go right off the paper. They are also rising faster. Health care costs are a major national issue. They are the #1 cause of personal bankruptcies. They are a major financial concern for retirees, Medicare notwithstanding. Health care outcomes overall are no better than other industrialized nations; indeed, in many respects, they are worse. So the belief that health care costs are NOT out of control would certainly be a curious one.
No it isn’t. That is in no way any kind of meaningful concept of “choice” in the context of health care. The insurance part of it shouldn’t need to be any kind of choice at all, since the fundamental purpose of health care coverage is to pay for medically necessary health care when you need it, period – no more, no less. And if it does so without question, without conditions, without demands for co-pays, what more do you need? The purpose of health insurance is to pay the bills, a pretty mundane and simple process. If it does that reliably and consistently, and at a low uniform cost for everyone, there’s no choice to be made. This is the quintessential argument for single payer.
“Choice” enters into it in the matter of your choice of doctor, your choice of hospital, and your choice of what treatment you want to receive. You don’t have complete scope of freedom on those real issues with private insurance, ever. Having a “choice” of different insurance plans, each of which is going to screw you in slightly different ways, and all of which are going to empty your wallet while doing so, is not a meaningful choice at all. And claiming that you’ve been deprived of “choice” because you can no longer buy a truly awful cut-rate plan whose primary goal is to be even shoddier than the rest of them and screw you over even worse is just so totally missing the whole point about the nature of health care.
Another respected health care economist is Uwe Reinhardt at Princeton, whom I’ve often quoted in these kinds of discussions. If more people listened to health care economists like Reinhardt instead of insurance lobbyists and crooked politicians some real progress might actually be made.
Just to further destroy the whole “but we’re paying for R&D” excuse, the following article is pretty good:
Pharmaceutical industry gets high on fat profits - BBC News?
“as the table below shows, drug companies spend far more on marketing drugs - in some cases twice as much - than on developing them”
Seriously, worth a look. Lays out just how many billions in profits the pharmaceutical companies are spending, along with how little they spend on R&D.
And that advertising budget is predominantly spent in the US, as it’s one of the only countries that allow drug companies to directly advertise to customers.
{kind=link}