I agree with pretty much all of this – and I really want to see single payer adopted.
I might suggest for #2 above that the median amount paid by employers for health insurance premiums be calculated and this be imposed as a per employee tax on all employers. Yes, this will be more expensive for companies without sponsored insurance plans, and those with less-than-average coverage. It would also be somewhat more expensive for those employers who are currently paying the median since they are paying pretax dollars now – but I’m thinking that extra amount might be offset by lower administration costs for the company. In any case, this is a place to start. Also perhaps these amounts should be prorated somewhat by insurance costs within the respective geographic region or industry.
Also institute a tax on employees similar to their share of SS tax. Amount to be determined.
The amount of all this should be calibrated to leave the typical employer and employee “whole” in terms of net income. My guess (and it’s only a guess) is that this would generate enough revenue to fund the single payer system.
In terms of #4 above, I’ve always imagined that any single-payer system would be matched with optional private insurance in the same way that many (most?) Medicare recipients buy supplemental insurance.
What do you mean by “hiding the cost?” For example, some people think that the withholding that is taken out of everyone’s paycheck is “hiding” the cost of income taxes, because Americans typically don’t get bent out of shape on a biweekly basis. These people think that prohibiting withholding and making people pay income taxes in one lump sum would make them feel the cost of taxes more; but it is plainly obvious that every American can easily see how much they pay in income taxes, either by looking at their pay stub or their annual W-2.
Then there’s the concept that certain things really are hidden from public view, like how much the military spends to support presidential travel. There are estimates of much much this costs, but there’s literally no budget line item that people can look at to assess whether it is too much or not enough.
Obviously, any single payer system will have a budget, just like Medicare or Social Security, that people can google and read about. So do you mean that people should “feel” like they are paying quite a bit for health care?
adaher, thanks for posting this more succinctly than I could. This is my big problem with the current single-payer push right now; it feels like a stump speech and not policy. The plan excludes a cost estimate. It (supposedly) does include an itemized list of what’s covered and what’s not; the bill is S.1804 for those playing along at home, but it hasn’t been released on the congress.gov website yet. The crucial details are lacking and yet people are jumping on board. Just because the plan calls for a single-payer system and single-payer systems tend to work generally does not mean this particular plan is necessarily a good or sensible implementation (see California’s recent proposal).
As a data point, I personally object to substantial wait-times such as what’s found in Canada for some procedures, so I would want to see a system cost in the neighborhood of 12% of GDP that covers everybody, with taxes or other mandated payments to match. Those parameters would then set an upper bound on what’s covered. My preference is more towards Bismark-style non-profit multipayer systems, but I’d be okay with a single-payer system without a “private option”. Different strokes for different folks.
I disagree that single-payer can work at the state level across the board. It can probably work fine in larger states, but I do not believe it can work in smaller, poorer states. To make it work in the smaller states, I think you’d have to allow the smaller state governments to engage in collective bargaining and at that point, I don’t see that as being particularly advantageous over a Federal system. It also tends to be more challenging for states to deficit-spend so states would need to run substantial rainy-day funds under state-based single-payer, policy which has its own own economic impacts.
The lesson the Democrats are taking from 2016 is that you shouldn’t run on white papers. You should run on big ideas without being forthright about costs, tradeoffs, and political difficulties.
I’m not sure they are wrong. Though I think what they will find is that Democrats are held to a higher standard than Republicans by their voters and by the media. And certainly the frontrunner is held to a higher standard. Neither Bernie nor Trump were ever frontrunners, so it is a mistake to infer too much about how their (largely empty) policy ideas were treated.
It’s almost not even worth having a debate at the level of the OP, because there is no policy to be debated. It’s just a vague aspiration.
In the sense that many mainstream media outlets believed him to have a good shot at the presidency. My reading of the coverage, and particularly the policy-related coverage, is that Clinton’s proposals were covered like they might one day be proposed in the actual government, while Trump’s and Bernie’s were not.
Anyway, none of this discussion matters. Theoretical propositions help us get to grips with reality, but the United States of America will never implement Single-Payer or Universal Health Care or any other sensible socialist system, any more than they will ban guns. It’s not worth thinking about either one.
A week ago I was trying to describe Hillary and I drew the analogy to an SF short Story from a paperback collection I have or had, but can’t find out anything about the story, probably 1950s. Anyway, authorities ( maybe the old professor who lives in a laboratory on the cliffs or maybe the weather service or the FBI ), are called out because a lightning strike hits the earth, dropping a small multi-coloured ball object, who then causes havoc by changing into absolutely anything to evade and deceive. It may be a baby, or a giraffe or a telegraph pole, or whatever: the point is that it is protean.
So, looking Proteus up, I came across this German professor who came over to America — either running from school fees from the Prussian authorities who provided his education or as a noble idealist persecuted for his socialism — and invented a tremendous amount of electrical knowledge. Charles ‘Proteus’ Steinmetz was the name he then chose.
However, he junked socialism once he reached those shores because…
Despite his earlier efforts and interest in socialism, by 1922 Steinmetz concluded that socialism would never work in the United States, because the country lacked a “powerful, centralized government of competent men, remaining continuously in office”, and because “only a small percentage of Americans accept this viewpoint today”.
It was a fair conclusion, even in those Wobbly days; and the same applies to health. The nature of Democracy means that all the tea-partiites and the Kochites and the ‘Plain People of America’ [ to go Myles na gCopaleen… ] will block it forever and ever, aided by the serious party masters like Cruz or Ryan, saving dying people from the moral delinquency of state control.
Better Dead than Looters.
Most countries fund their health care with taxes that hit everyone and which are easy to understand. Sanders’ plan raised some money here and there with various taxes, most of which the public wouldn’t see and others were which direct but hit only the top 1%. That’s a very novel way to fund a single payer system. It’s also completely unsustainable and probably wouldnt’ even work in year 1.
Those programs don’t have a budget. They are IN the budget, you can see how much is spent, but they are not controlled. They are open ended commitments. The single payer plan should not be. I’m not going to say that’s a requirement for me, but if the program is open ended, it has to be clear that this comes with an ever increasing social insurance tax to fund it. Something like this can’t be allowed to run a deficit.
The big ideas part is right, and you don’t have to get specific right away. I’m not demanding that they get specific right the hell now when they can’t pass it. I’m just discussing the details that will be necessary to get right before they actually do try to pass it in 2020 or beyond.
Of course, once they start campaigning on it, anything they say(or fail to say) can and will be used against them. One key talking point which my side is already using is that pretty much everyone now agrees that we need to get rid of ACA.
Well, I will say that America’s Military Spending ( no judgement ) appears to be easily and fully funded by the state.
Don’t see why the same mechanism can’t support other projects.
Even though, as happens, the generals feel they are underfunded and want more taxpayers’ money.
This presumes they will try to pass something in the conceptual space you’re describing. I very much doubt it. The lesson of healthcare politics is that people like the abstractions and hate the details. It doesn’t really matter what the details are because most active voters are happy with their employer-provided insurance or Medicare.
What we will see in reality is the addition of a public option for ACA marketplaces, the expansion of Medicaid and/or Medicare, or both. As to those actual policies, I don’t think your conceptual questions make much sense. Medicare, for example, will be no more or less transparent than it currently is if expanded. It is paid for with a dedicated funding stream, though obviously your definition of “paid for” is going to vary. Etc.
Because defense spending is for a specific purpose in a specific time and can be cut very easily if circumstances justify it. It can also be cut fairly easily if we have no choice due to budget realities. You can rest assured that no country will ever bankrupt itself supporting a peacetime military. Every other nation has squeezed their defense budget when the rest of their budget got too big, and we will be no exception.
Nations WILL bankrupt themselves over popular social insurance programs, however. Which is why more care is needed when implementing them.
I agree that changes to ACA are probably what will actually happen, such as a public option.
And Medicare’s funding stream is exactly what I want to see for single payer. I mean, if you want Medicare for all, do Medicare for all. Boost the payroll tax as much as necessary to pay for the larger population.
Let’s just say for argument’s sake that someone proposed a single payer system that taxed the sale of each share of stock by some tiny fraction of a cent, and that it was generally accepted by fiscal experts that it would raise sufficient funds for this purpose. Would you oppose this revenue source on the basis that regular people didn’t see or feel the tax, even though all such excise taxes are ultimately passed on to the general public?
That’s stupid.
I know what you mean, but it isn’t really accurate. Medicare has been subject to a sequester of a few tens of billions of dollars since the supercommittee failed. I call that “being controlled.” But in any case, spending on Social Security and Medicare isn’t hidden. It’s information that can be found in one fraction of a second on Google.
Are you really using these terms of “hiding the cost” to mean what you say elsewhere in your OP, that you favor capping health care costs and cutting services if required to make sure we meet arbitrary estimates of how much we ought to spend?
I agree with your point here, but really I think you’re seeing this in a short-sighted way. The establishment of a set funding mechanism for a certain activity is a risky thing over the long term. Take for example, using gas taxes to fund road maintenance. When that policy was proposed, nobody ever thought we’d have millions of cars that get 50 mpg or the (slow) mass adoption of electric cars. Now road maintenance is underfunded. Meanwhile, for many years (and I think this continues), the Patent and Trademark Office charges fees to its users and accumulates surpluses, which it wishes to keep rather than cutting costs to the users. Or in another case, some have advocated pegging defense spending at an arbitrary percentage of GDP, for what reason I have no idea – are we more threatened as a country in a booming economy, but less threatened during recessions? All of these examples show the silliness of pegging dollars in to dollars out under a fixed an inflexible formula.
There are some situations in which dedicated revenue streams make things politically more palatable, but really I don’t think it’s smart policy.
The Sanders plan includes a transition period with a strong public option with increased premium subsidies, and a Medicare buy-in for people over a certain age, with reduced cost-sharing under Medicare. I would not be surprised if what we end up with is just the transition.
Its much easier to just engage in name calling you know. Now I have to actually research my opinions.
What are the big concerns about single payer?
[ul]
[li]Longer wait times[/li][li]Restrictions on certain treatments[/li][li]Poorer outcomes for certain illnesses[/li][li]Health care in the hands of government officials (what if officials hostile to single payer come along, everyone’s health care suffers)[/li][/ul]
Wait times - most of this is based on Canada, which does have issues with wait times due to how their system is structured.
Lots of nations with UHC have low wait times according to that (Belgium, France, Japan, Germany, etc)
Restrictions on certain treatments - this is covered in point 3 below.
Poorer outcomes for certain illnesses -
The US has poorer outcomes too. It isn’t a one way street.
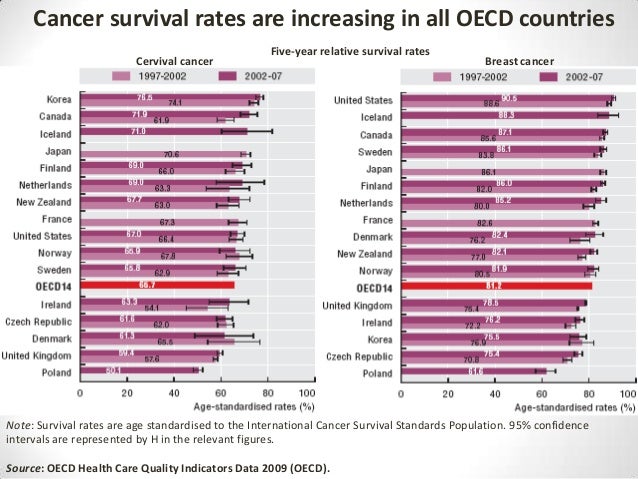
For cancer, the US is top for survival for breast cancer, middle of the road for cervical.
Our cancer survival rates are high, but not the highest. The different seems minor overall.
I do worry about point 4. What if the tea party takes over and cuts everyone’s health care. I can’t just quit my job and find a job with better health benefits if that happens like I can with the current system.
Groups like PNHP or HR676 have funding measures for single payer. Currently about 50% of medical bills are paid by the government. Under single payer maybe/hopefully it’ll only cost 85% as much, which means we need an additional 35% of the health care system (about 6% of GDP) as taxes to fund it.
Usually this is a mix of payroll taxes and supply side taxes. Maybe a 10% payroll tax split between employer and employee with no cap (so if you earn 50k, you pay $2500 a year and your employer pays $2500 a year). Plus you have the supply side tax hikes.
An example of funding mechanisms can be found here on page 5.
The UK has a good system IMO. They cover everything that costs 35,000 pounds per QALY added. Which means (from what I know) virtually everything is covered. The only things not covered are certain highly expensive medications for terminal patients (a cancer drug that costs $100,000 and extends life by 2 months) and maybe some highly expensive treatment for elderly people who aren’t expected to live longer than another year or two.
Basically, my impression of systems like the UK NICE system (someone correct me if I’m wrong) is that all it means is that extremely expensive therapies will not be given if you are terminal. Extremely expensive therapies will be given if you aren’t terminal (you have a car wreck at 35 for example), and less expensive therapies will be given if you are terminal.
My impression is about 99% of medical interventions are covered under the UK NICE program compared to the US, so it should be a non-issue if the debate were factual (and lets be honest, it won’t be). If I’m wrong, please correct me.
A bigger issue IMO, is that therapies that are ineffective will not be covered in a well run system. Certain surgeries are expensive and totally ineffective. So if you have a back problem and you tell the doctor ‘I want back surgery’ and the doctor says the health system won’t cover it, that could cause some upset. But the reason it isn’t covered is because clinical trials show it is ineffective, all it does is cost money. However this will be a major issue of contention for people under a UHC system (of course we have that now, only difference is insurance denies anything it can, not just ineffective therapies).
Thats fine. Australia has a good system, they have Medicare for everyone and you can get private insurance on top of it. No reason that wouldn’t work here.
I’d like to point out that single payer is not the solution to our problems. We spend 18% of GDP on health care. If we had single payer, we may ‘only’ spend 16-17% of GDP. That still makes us way more expensive than other nations. Australia which has a single payer system plus a private system on top of it costs 9% of GDP. The Netherlands which has a multipayer system (basically Obamacare on steroids) only spends 9% of GDP.
Getting medical costs under control is the #1 priority IMO. If single payer can’t do that, it won’t fix the issue. If a system other than single payer can do this and is more politically feasible, we should support that instead.