Wow. I teach this stuff. Where do I begin? Re: other countries. Victor Fuchs, 1970s era book, “Who Shall Live?” Interesting demographics- the primary cause of death in African Americans (at the time) until age 45 was homicide. The primary cause of death in white males until age 35 was accidents, primarily vehicular. The difference in cancer, cirrhosis, and heart disease between Nevada and Utah exceeded 200-400%. One suspects there are certain cultural differences between Utah and Nevada. So. We may have one of the finest HC systems in the world, but, as a culture, we just have a predilection for doing crazy dangerous, self-destructive stuff. Which cuts down our life expectancy, compared to nations spending less. We attempt to save premature births many others countries don’t- inflating infant mortality.We have the grey tsunami, as baby boomers age, and fewer and fewer taxpayers are paying in to cover their MUCH higher HC costs. We don’t tax HC benefits as income, a relic of WWII. We are seriously uncomfortable with death, and will pay almost anything to avoid it. Yes, 23% of the HC spend is for about 2% of the population, but in the next year, about half of that 23% is made up of individuals from the previous year’s 23%.(Seriously- about 1% of the population has ever heard a death rattle, or even knows what it is, when once it was simply a fact of life for all. Its amazing how many oncologists are Asian-Indian- I guess hinduism makes you more comfortable with dying as a step to the next cycle of life). When the time finally comes, I can’t tell how many times I and many other colleagues have been left to deal with it, because the family didn’t want to witness/deal with it themselves. And somewhere in there, we as a people have come to see health care as a right.
So- as the system works through the baby boomers (in the 60’s, there were 35 people to pay each person’s social security- that number’s down to about 2)- we WILL see the system break in places.
Predictions:
taxation of benefits as income
Universal HC insurance, to get everyone paying into the system, not to provide care to the young who rarely need it. If you don’t sign up for Medicare part D as soon as you are eligible (even if your premiums and copays would exceed your current drug costs) you will pay a penalty of a 1% increase in your premium for each month past your eligible date, and that penalty is for life.
Health care rationing- already a fact in many places, under different names. A lot of states limit Medicaid recipients to, say, 5 prescriptions a month.
Ever higher deductibles and co-insurance, and higher premiums.
Much more care at home, shifting the costs to the family.
Actually, most of the increase in HC has been absorbed by business, state and federal government. HC care costs as a % of household income has remained remarkably steady for decades, at the 5-6% mark- because households VOTE. BUt that is most assuredly starting to change, and is only going to get worse. Its called “risk sharing”.
Encouragement of DNR orders.
A lot more hospice, for a lot more conditions.
Oh, and regulation of “life-style diseases”. (this is where the battle over HC as a right is at right now). Some employers have made it a condition of employment that you don’t smoke. You smoke, you get 6 months to quit. If a hair snip shows nicotine, you are out of a job. Georgia, I believe, made it a condition of continued employment for all state employees whose Body Mass Index => Morbidly Obese to enroll in a weight loss program and so progress or forfeit employment.
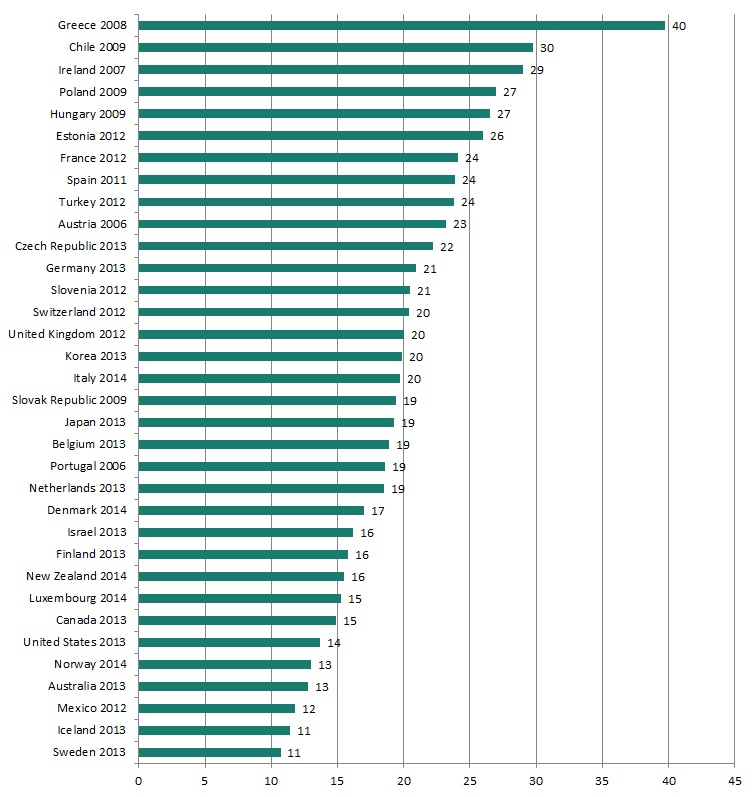
You can’t get a liver transplant if you drink. The list goes on. We have as a % of the population (in 2009) 33.8% with a BMI over 30. The next nearest in “western industrialized nations” was New Zealand, with 26.5%. Australia and Canada are at 24%, and France and Germany are 12 & 14%, respectively. One reason we do twice as many bypass operations as the next closest country.
So expect the system to become less willing to provide care for problems related to personal choices, as unfair as that may sound or be.
Finally, although the sense here sounds almost axiomatic that we cannot move to single payer health care, the reality is that administrative costs in the public insurance in the US (Medicaid/Medicare) are 4.1%, while the administrative costs in the private sector are more than twice that. A lot of Medicare is now managed care, run by commercial entities. SIngle payer may just sneak up on us.
Oh- and we may institute another layer to our HC legislation, much like the UK- new drugs, procedures, and devices are subject to an analysis of their relative cost-effectiveness compared to current options, and unless a clear advantage is evident, in many countries, that treatment will not be approved for use in said country, or only through direct private pay.
The emerging consensus across the world seems to be that access to care should be determined by need, and cost determined by ability to pay- with a growing “distancing” from support for life-style diseases as an undercurrent, moving away from HC as a right.
Given that HC has come to be described as “permanent white water”, that’s about as far as my crystal ball goes.
The only good news? For decades, I have taught that the rate of health care inflation exceeds the rate of inflation for everything else in the economy. I can’t say that anymore. The new leader? College Tuition.
{kind=link}