This. I am a post acute hospitalist, and every day I order treatments that while technically are medically indicated, they won’t do anything useful. Unfortunately a significant percentage of people who have medical power of attorney for patients with end stage disease don’t realize that there comes a point when continued treatment just doesn’t do any good. None of us will get out of this alive. I think we do need some kind of “death panels.” They would prevent things like a person with end stage dementia who develops pneumonia going to the ICU on a ventilator and receiving IV antibiotics that cost several thousand dollars a day. The best case scenario for a patient like that is that they go back to being in a vegetative state, only to get another infection a few weeks or months later. Unfortunately this scenario and others like it are far to common.
“How we used to die; how we die now” … just one person’s opinion but they have some good points about end-of-life care.
Well, that’s lovely, but you do realize that sterile saline is used in surgeries. Why on earth would I want to DIY my own saline? What, I’m going to sterilize some ziploc baggies at home and then bring them in and be all, “No, use these!” :rolleyes:
It’s about 1% on average, or should I say 1% is the healthy amount. This can go up to 3% if you just had a particularly salty meal. Surprisingly, and this might shock all of you, the purpose of the contents of the IV bag isn’t to put salt into your system … rather … to put water into your system. An EMT friend of mind said every patient she comes across is dehydrated, pretty much no exceptions.
I was trying to be facetious, where the article was complaining about how much higher the costs of medical supplies are than what can be bought over the internet, I was complaining about the high cost of medical supplies over the internet over what can be prepared at home. Just get a glass off the shelf, fill it with water, and administer orally … no salt needed (you might want to rinse the cat hair out first).
This illustrates another reason health care costs so much, people just will not educate themselves. None of us drink enough clean water.
Summer’s coming, here’s a list of the symptoms of heat stroke from the Mayo Clinic. Alternately, drink lots and lots and lots and lots of water … a truly precious body fluid.
My company doesn’t sell health insurance, although we do process enrollments and claims on behalf of some governments and provide some managed care functions to private agencies.
We have to report to at least 100 different federal and state agencies. Then we have to satisfy audits (I specialize in explaining the automated processes to auditors and producing software to provide data and validate the numbers). If no one is doing an audit, how does the consumer or client know if they are being overcharged or if mistakes are being made or if someone is engaging in various forms of fraud?
Then there are issues of monthly reporting and data exchanges with CMS and its agents. There are also involved data requests from various Attorneys General to satisfy investigations of drugs, treatments, and programs.
There are drug rebates to various states. Many entities work out rebate agreements between drug manufacturers and clients. They, usually government entities, recoup some of their expenditures on drugs directly from manufacturers. These are processed and billed quarterly, with invoices going to various manufacturers, payments being collected, and disputes being resolved.
You need to have people who interface with customers to answer questions about policies and charges, or provide information about constantly changing plans and coverages. You need to have the same thing for providers who call with questions.
I don’t see how you get out of administrative overhead. You can move it around a bit, but it can’t be eliminated entirely as long as some measures of accountability, review, and dealing with customers are required. It’s a sub-business within itself. A necessary one.
I can’t even imagine how, regardless of design or government, there isn’t a conscientious and detailed review of spending, payments, rebates, who is spending how much on what, and the like. You can’t get rid of that and still have a system that is accountable to the customer and to the taxpayer.
Or it’s to put medication into you via IV.
Sorry, saying “1-3%, more or less” is NOT acceptable for something being injected directly into your veins. Which is distinct from “oral rehydration” a.k.a. "having a drink of water.
And the week my system was in such an uproar I couldn’t even hold water down IV fluids were essential - if I had not had them I would have died. Not everyone is able to drink sufficient water if they’re injured or ill enough, and some medications need to be administered directly into your circulatory system. Sorry if you don’t understand that, but like you said, a lot of people could use some additional medical education.
“Drink enough water” is an entirely different matter than “preparing saline for IV administration.”
I concur that who ever said “1-3%, more or less” probably doesn’t know why salt is thrown in and why it needs to be the 1% I specified. Still the item retails for $5, that’s how much Wal-Mart has to sell it for to make a profit. That includes manufacturing, packaging, transportation and stocking the shelf. Pretty much the same for a hospital, the item sits on the shelf outside the operating room and retails for $5 and that includes hospital profits.
Well, that item shows up on your bill for $55, a 1,000% markup from retail. The question is can we find ways to cut this expense to the patient.
Please save me the long list of why the the IV costs more than $5 at a hospital, I’ve a business myself and take every opportunity to increase profits. If the hospital can get that price, I see no reason why they shouldn’t.
Understandable, your money’s no good to you if your dead. You can either hope you have enough money or buy health insurance. Do we as a society have a responsibility to look into these charges at a time when you maybe aren’t able to look into them yourself?
According to thismedicare spends $50 billion a year on the last 2 years of a person’s life. Something like 2.2 million people in the US (roughly that number) die per year and were 65+ at the time, that works out to about 24k per person for the last 2 months.
Something to look into, but in light of our 3 trillion health care system it is just a small part of the solution.
Part of the mark-up in hospitals is to cover the cost of treating the uninsured and those who skip out on their co-pays. SOMEBODY has to pay for stuff, even if the patient skips town. The current solution is to everyone else pay more to cover for that loss.
That is definitely part of the mark-up.
So, if we covered everyone via universal coverage we wouldn’t have the uninsured patient problem anymore, or at least much less of one.
That would help cut the costs of health insurance, but why isn’t anyone actually looking to cut health care costs?
Part of it is that truly cutting health care costs requires cutting billions in income for powerful industries who will not take it sitting down, and it will go against the ideological leanings of much of the country.
Forcing insurance companies to compete with a program tied to medicare (or replacing insurance altogether with medicare)
Rx drug negotiations
Rx drug reimportations
Eliminating unnecessary and unproductive care
Making prices of procedures, medical goods, etc transparent
Allowing the government to negotiate prices
Giving the government a giant hand in reshaping the health care system
etc.
There are small programs here and there, but on a national level nobody is doing anything to make our health care spending more in line with other OECD nations.
The problem lies in the difficulty of identifying ex ante which years are going to be the last two.
Shifting the cost of charity care from one payor to another may affect questions of fairness, but it doesn’t reduce the cost to the system.
There are higher costs baked into our system at all levels. Wesley Clark is correct that significant cuts in health care costs would require the government to impose significant cuts in the income of medical professionals (to the much lower levels paid in the OECD), and that ideologically, we trust our doctors more than we trust our politicians, which means that cuts of that sort could never happen.
Moreover, no other country has ever made cuts of that sort. Or any sort. No one has ever been successful in cutting health care costs. For a relatively short time in the past, the OECD countries did better than the US at restraining cost growth, which is why their systems are now less costly than ours. As of now, though, the US rate of health care cost growth is about the same as Europe’s. In other words, we could adopt all of the features cited by Wesley Clark and make our system as much like an OECD country’s as one might wish to, and it still wouldn’t slow the growth of our health care costs, let alone reduce them.
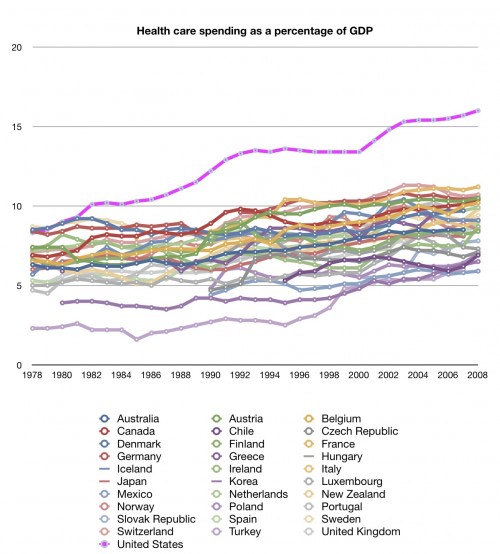
Between 1980 and today the US’s spending on health care has grown from about 9% of GDP up to 18% today. In pretty much every other OECD nation it only grew 2-3%, going from maybe 7% in 1980 to 10% today in some countries. Some countries kept their spending as a % of GDP stable all those years. Israel has kept their spending at a stable 8% of GDP for the last 30+ years.
I don’t know why our health care inflation was so much higher the last 36 years, or if anything realistic can be done to bring them back in line.
Someday they’ll come down, and it will not be a soft landing.
It may, if the costs can also be shifted in time. For example, many uninsured don’t show up at the doctor or ER until the problem has gotten to the critical point; if you can get them at an earlier stage of the problem process, it may be much cheaper to solve. For example, keeping diabetes under control is generally cheaper than getting it back under control after a diabetic emergency, while early-stage cancer requires less intervention than later stages. That’s not true for every disease or medical condition, but it’s true for enough to move the cost line.
In the single payer system where I live (Canada), medical offices only have to report claims to two different agencies: the provincial health insurance commission for the great majority of patients, and to the Workers’ Compensation Board, a different provincial agency, for treatment for work-related injuries. In practice, WCB is not a large portion of payments for medical care in the province. There is therefore only one set of codes needed, not over 100.
Here, the [del]consumer[/del] patient does not have any involvement in payment, since there are no co-pays or deductibles. The two clients (insurance commission and WCB) can and do conduct audits.
The provincial governments have worked out a system for uniform drug costs across the country, for drugs used in the hospitals, by using their combined purchasing power, just like WalMart.
Since coverage of medical matters is uniform and universal within a province, there is no need for that function in our system. [del]Customers[/del] Patients never have to ask those questions, since payment is made by the medical commission directly to the doctor or the hospital.
The provincial insurance commission is the one that sets the terms, so there is no need for this function in our system.
Every system has administrative overhead. But the amount of administrative overhead multiplies the more complex your system. Administrative overhead in a single-payer system is much lower than a multi-payer, private insurance system.
Agreed, any system needs an effective audit system. However, the more complicated your payment system, and the more payors there are, the more complex and expensive the audit function becomes. Here, the medical insurance commission performs regular audits within the medical system, and has the statutory power to claw back over-payments. Because there is only one payer and one payment structure, audits will be much simpler and less expensive than what you are describing.
You are required to deal with insurance companies in some countries.
My understanding is that in Germany, Australia and France, coverage is provided by insurance companies, but under strict government regulation.
Those countries don’t have a government system of single-payer, unlike Canada and the UK. (I’m open to correction on this, but that’s my understanding from previous threads on this issue.)
I think a big/huge part of it will be outsourcing of health care combined with people treating their own conditions.
People will go overseas for long term care, surgeries, importing drugs, etc. and more and more people will resort to treating their conditions at home using the internet.
I think those 2 things will take some pressure off. But if in 20 years people are looking at $100,000 bills for a 30 minute appendectomy and insurance refuses to cover it, I’m not sure what will happen.
What would happen if we built a few new medical schools and gave out lots of medical school scholarships? That could help more people become doctors (and possibly other medical professionals). The “new” students would still have to meet requirements (e.g. pass all their classes and exams, etc.), but there would be more opportunities for capable students to get their chance. Then, we could have a glut of licensed physicians driving down salaries and therefore medical costs. Need a doctor? Go down to the welfare office and pick one of the doctors hanging out out front with a “Will diagnose for food” sign. He’s fully licensed, but so desperate for income that he’ll do that procedure for $39.95 and a bus ticket home.
Why do you think that anyone isn’t trying to cut health care costs?