New Jersey had two straight days of under 2000 new cases. First time since November 3rd.
2/14 = 1798
2/15 = 1222
Also I got tested yesterday as a pre-check before surgery Friday. Results were Negative!
New Jersey had two straight days of under 2000 new cases. First time since November 3rd.
2/14 = 1798
2/15 = 1222
Also I got tested yesterday as a pre-check before surgery Friday. Results were Negative!
That’s great news, but it’s also over Presidents’ Day weekend, so both testing and reporting are probably depressed.
And good luck on your surgery! Hope it’s as uneventful as your test.
Britain gets tough over travel restrictions:
Four air passengers have each been fined £10,000 for failing to declare they had travelled from a “red-list” country, West Midlands Police has said.…
…Birmingham Airport is one of five in England where people requiring hotel quarantine can enter the UK.
Those who fail to self-isolate as required face fines of £5,000 to £10,000, while anyone who lies on their passenger locator form about having been in a country on the red list faces a prison sentence of up to 10 years.
j
Looks like the US will clock in at just under 500k deaths today. 499,991. 
Although the story contains a glaring non sequitur.
Those who fail to self-isolate as required face fines of £5,000 to £10,000, while anyone who lies on their passenger locator form about having been in a country on the red list faces a prison sentence of up to 10 years.
Four air passengers have each been fined £10,000 for failing to declare they had travelled from a “red-list” country, West Midlands Police has said.
They didn’t just fail to self-isolate, they failed to declare - i.e. they lied about where they had been. So why just a fine, and no prison sentence?
I guess “up to” 10 years can include zero years?
Sure, there’s always discretion to impose a lower sentence. But it’s hard to imagine that there’s really much scope for variation in lying about where you have been, other than repeat offences. If it is policy to impose prison sentences, what kind of lying does attract a prison sentence, and in what way was the kind of lying these people did so much less dangerous that a milder punishment was warranted?
110,035,633 total cases
2,429,811 dead
84,851,754 recovered
In the US:
28,381,220 total cases
499,991 dead
18,479,418 recovered
Yesterday’s numbers for comparison:
IANAL. I think that the penalties apply to the Legislation, but the offence applies particularly to the regulations. FAIK, there may be heaps of other regulations or other offences that are covered by the same range of legislated penalties.
And perhaps, in line with sentencing guidelines, the prison terms will only be applied to the kinds of offences that normally justify prison terms – perhaps 10 years for deliberate behavior causing actual death of a health worker.
Likewise IANAL, but a couple of thoughts:
Police chiefs have followed a system called “The Four Es”. Before fines are issued to rule-breakers, police will first:
- Engage with people, to ask why they appear to be breaking the rules
- Explain the law, stressing the risks to public health and the NHS
- Encourage them to change their behaviour
The fourth “E” is “Enforce” by issuing penalty notices, as a last resort.
So perhaps the thinking here is just a warning shot - these were the first penalties I am aware of, and the rules had been in place for less than 12 hours at the time of the offence.
Sir Keir Starmer has criticised the proposed maximum 10-year jail term for people lying about their recent travel history as an “empty threat”.
The Labour leader said “pretending” judges would sentence anyone to that long in prison “wouldn’t help anyone”.
Ministers have said the public expects strong action and the maximum sentence reflects the seriousness of the crime.
But critics, including ex-Supreme Court judge Lord Sumption, have argued lower tariffs exist for sex offences.
j
FWIW.
Paywalled, but the Atlantic allows four free articles per month to non-subscribers.
Bare bones highlights:
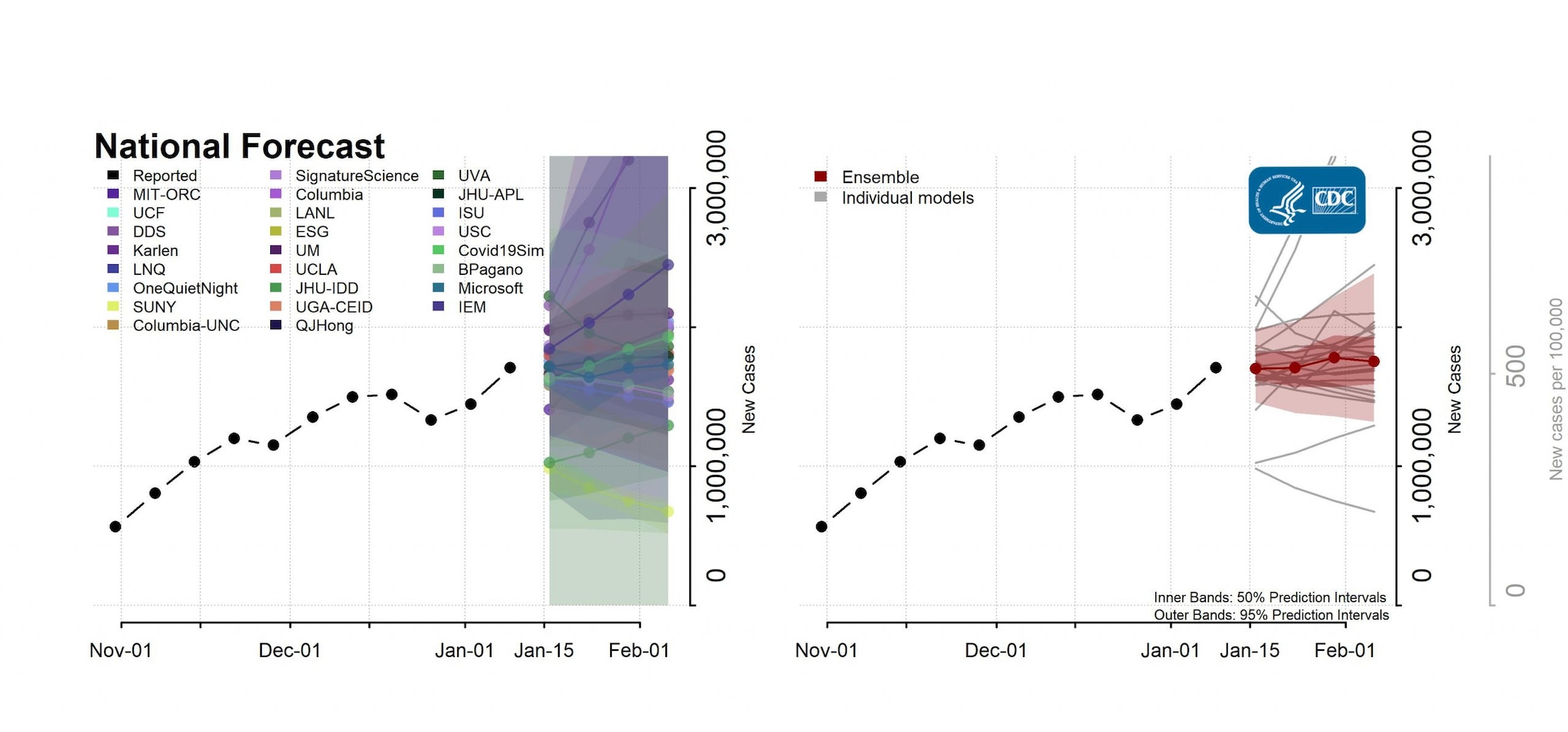
One month ago, the CDC published the results of more than 20 pandemic forecasting models. Most projected that COVID-19 cases would continue to grow through February, or at least plateau. Instead, COVID-19 is in retreat in America. New daily cases have plunged, and hospitalizations are down almost 50 percent in the past month. This is not an artifact of infrequent testing, since the share of regional daily tests that are coming back positive has declined even more than the number of cases. Some pandemic statistics are foggy, but the current decline of COVID-19 is crystal clear.
What’s behind the change? Americans’ good behavior in the past month has tag-teamed with (mostly) warming weather across the Northern Hemisphere to slow the pandemic’s growth; at the same time, partial immunity and vaccines have reduced the number of viable bodies that would allow the coronavirus to thrive. But the full story is a bit more complex.
1. Behavior: Maybe Americans finally got the hang of this mask and social-distancing thing.
“If I were ranking explanations for the decline in COVID-19, behavior would be No. 1,” says Ali Mokdad, a global-health professor at the University of Washington, in Seattle. “If you look at mobility data the week after Thanksgiving and Christmas, activity went down.”
…2. Seasonality: The coronavirus was perhaps destined to decline this time of year.
Behavior can’t explain everything. Mask wearing, social distancing, and other virus-mitigating habits vary among states and countries. But COVID-19 is in retreat across North America and Europe. Since January 1, daily cases are down 70 percent in the United Kingdom, 50 percent in Canada, and 30 percent in Portugal.
This raises the possibility that SARS-CoV-2, the virus that causes COVID-19, is seasonal.
…3. Partial immunity: Is the virus running out of bodies?
The coronavirus needs bodies in order to survive and replicate, and it now has access to fewer welcome hosts. Fifteen to 30 percent of American adults have already been infected with COVID-19, according to CDC estimates. Since people recovering from COVID-19 typically develop lasting immunological protection for many months (at least), the number of antibodies swirling around the U.S. population may naturally constrict the original coronavirus’s path forward.
America’s seroprevalence—that is, the number of people with coronavirus antibodies from a previous infection—is not randomly distributed across the country. Instead, immunity is probably concentrated among people who had little opportunity to avoid the disease, such as homeless people, frontline and essential workers, and people living in crowded multigenerational homes. It might also include people who were more likely to encounter the virus because of their lifestyle and values, such as risk-tolerant Americans who have been going to eat at indoor restaurants.
What I’m describing here is not herd immunity. Nothing is herd immunity, really. But it is partial immunity among the very populations that have been most likely to contract the disease, perhaps narrowing the path forward for the original SARS-CoV-2.
…4. Vaccines: The shots work.
COVID-19 cases started falling in January, when almost nobody outside of the health-care industry had been vaccinated. So vaccines probably don’t help us understand why the plunge started . But they can tell us a bit more about why the decline in hospitalizations has accelerated—and why it’s likely to continue.
…That’s a lot of messy arithmetic. But the upshot is simple: Even if the rise of new variants slows the decline in cases, it is unlikely to lead to a sharp rise in mortality and hospitalizations. Although the pandemic isn’t over, we have perhaps reached the beginning of the end of COVID-19 as an exponential, existential, and mortal threat to our health-care system and our senior population.
Thanks. Your analysis makes more sense than the news article. The notion that it’s really public policy that anyone could face any significant prison time for this seems pretty implausible in a world where there don’t seem to be harsh penalties for any kind of risky behavior by anti-masker deniers.
I just ran across this interesting paper.
https://www.pnas.org/content/118/8/e2021830118
I’ve been wondering, ever since the announcement of “super spreaders” and super spread events, whether it is possible to identify individuals most likely to be super spreaders and maybe mitigate their ability to spread. This paper is not a definitive study, but it does seem to identify the characteristics of individuals that exhale more aerosols than the general population and provide some potential mitigation paths.
It may also provide some insight into why the very young don’t seem to be super spreaders as often as adults.
Here’s something new - anybody out there up for being paid to be infected with COVID?
No Joke:
Up to 90 volunteers aged 18 - 30 years will be exposed to Covid-19 in a safe and controlled environment to increase understanding of how the virus affects people
Backed by a £33.6 million UK government investment, the first-of-its-kind study for this virus will involve establishing the smallest amount of virus needed to cause infection, which will give doctors greater understanding of Covid-19 and help support the pandemic response by aiding vaccine and treatment development.
To put a little context on this development, here’s the relevant paragraph from the Declaration of Helsinki (“Ethical Principles for Medical Research Involving Human Subjects”):
- Medical research involving human subjects should only be conducted if the importance of the objective outweighs the inherent risks and burdens to the subject. This is especially important when the human subjects are healthy volunteers.
Which tells me that this work can only proceed if an ethics committee is convinced that this approach can provide valuable information which cannot be obtained in the sorts of studies which have already been performed in the licensing of vaccines - ie, studies in which the vaccine is used to protect subjects “in real life”. There is a clue to one such benefit at the end of the press release:
[Chief Scientific Officer at hVIVO, Dr Andrew Catchpole said:]
…This study is a key enabling study to establish the Covid-19 challenge model and determine the lowest possible dose of virus required. Data from this study will immediately facilitate the challenge model to be used for vaccine efficacy testing as well as to answer a wide range of fundamental scientific questions that are not feasible with traditional field trials, such as exactly what type of immunological response is required to confer protection from re-infection.
j
ETA - if I can find a protocol, I’ll share a summary
Aye; despite the declarative title every entry is peppered with qualifiers: might, probably, may be, etc.
I wonder about the impact of these storms. Theirnhas been a whole lot of hard core social distancing going on. I haven’t so much as laid eyes on someone outside my household in a week, and there are millions more like me. My perhaps naive hope is that this hard reset will make the impact of vaccinations more dramatic. As the virus attempts to reestablish itself (as it surely would, without mitigation), the blocked potential chains of transmission will slow that down. And the slower it goes, the more people get vaccinated, the more it gets blocked.
These Human Challenge studies might answer some fundamental questions about the most effective way to vaccinate.
Current practice is based on trials that have a fundamental weakness: they compare and test and control group and then rely on community exposure, which can be highly variable and difficult to quantify. So the trials require very large numbers of participants to ensure some are exposed and even then the results for some age groups may not be conclusive because of the low numbers.
Some countries have decided that there is not enough evidence that the Oxford AZ vaccine is effective for the over 65s. This is contentious, they are all interpreting the same data.
Human challenge trials may fill in the gaps in the data on vaccine effectiveness, dosage, etc very quickly. Starting with 18-30 years olds is a pretty safe because the raw data on mortality suggests this age group is at very low risk from Covid infection.
Human challenge trials with volunteers is a long established practice amongst the student community and medical research institutions in London. Being paid for spending two weeks in a room watching TV and playing video games and undergoing various tests is regarded as easy money.
I’m guessing (see what I did there) that if every statement were declared with categorical certainly, you wouldn’t like that either.
This thing has many bumfuzzled. Sorry for the highly technical language.
The slowdown in commerce will certainly help. As will the virtual cessation of folks’ visiting one another. At the same time I imagine the vaccination effort in the affected areas has also ground to a near halt.
And all of those 3 things will restart more or less in sync with a wobbly first few days before pre-storm habits return.
![]()
{kind=link}