I’m struggling to stay GD-worthy and within my ‘energy envelope,’ but …
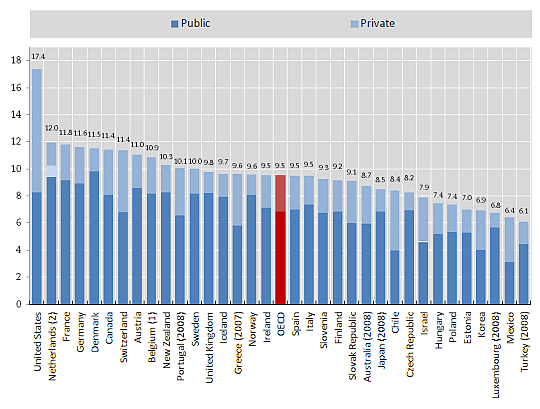
As others have implied up thread, the 18% of our GDP number attributed to healthcare is the bottom line result of a laundry list of “whose ox gets gored” if and when we get serious about UHC in this country.
Meaning – obviously – that somebody gets every single one of those dollars, and – humans being humans (and, perhaps more appropriately, Americans being Americans), ain’t nobody willing to let one of those dollars go.
Which speaks to how structural our health care crisis is, and how intractable it is. We probably do basically every single aspect of it wrong, but it is thoroughly institutionalized, calcified, and entrenched.
Phasing in measures that wring money out of the hands of stakeholders seems like it would have to be both painful and non-negotiable – a decree from on high.
But even selling well-funded stakeholders, with powerful lobbies, on the mere idea that they may have to tighten their belts for the overall good of the country is difficult.
Another thing that, IMHO, simply must be in the consideration set is to figure out all the drivers/social determinants of poor lifestyle (largely, diet and exercise) factors that contribute to the costs of delivering health care in the US.
A decade or so ago, I was traveling in Central America. In no end of little kiosks through every little town where I walked, they sold nothing but garbage processed foods. Young children walked the same dirt roads that I did, seemingly all clutching a big, BIG bag of chips in one hand and a big, BIG bottle of soda pop in the other.
I just kept thinking how economically unsustainable this would be, particularly in poorer countries committed to providing UHC.
And then I realized that … only a matter of degree separated those countries from our own.
This one, to me, feels like a “landing a man on the moon” or “Manhattan Project” thing that will take an extremely bold President – with lots of political capital and the enthusiasm to spend a chunk of it on day one – to even get rolling.