I know the experience of pain is highly subjective. But because of that, the pain level reported can be highly variable. On the one end, you have the Black Knight from Monty Python and the Holy Grail – “Tis but a scratch.” “A scratch? Your arm’s off!”. On the other end, we probably all know someone whose pain level is near the max with almost any complaint – “I have a hangnail, and let me tell you, you’ve never experienced such agony in your life!”
It seems to me that the experience of pain might cause some physiological effects – a change in blood pressure, or electrodermal response, or the like. It also seems that a more objective measure of pain could help with diagnosis or treatment.
So is it theoretically possible to more objectively measure how much pain someone is in?
I doubt it. As you observe, it is highly subjective. I review medical records all of the time as part of my job, and then speak with the people. Different people with very similar medical findings will describe very different levels of pain. Admittedly, these medical records do not attempt to objectively quantify the level of pain. Moreover, folk claim to perceive pain from non-physiological conditions.
It has long ceased to surprise me when someone sits there and calmly states, “Yes, I am currently experiencing pain at a level of 10 out of 10”, after just having been told that 10/10 pain is the worst imaginable, and would cause you to rush to the ER!
Like you said, there might be some physiological signs of distress, but I’m not sure they would identify pain as opposed to anxiety, etc.
I have a very high pain threshold. It isn’t that I don’t perceive pain, but I just am able to ignore it pretty well. Which can be good or bad.
The only way to measure it objectively would be to first subject them to a 1 (stepped on a lego), then a 10 (skin burnt by direct flame), then ask them where their complaint pain was in between - so, how was your hangnail in between that 1 and 10?. But there’s no ethical way to do that.
I recall reading a report about a study that did precisely that. Unfortunately, I can’t recall where i read it, or how they did it. But I think it was a “standardized” pain. I don’t think you could use the same number scheme on a headache as on a kick in the balls, but I could see comparing headaches.
That it’s subjective ought not to be a problem. We have a highly detailed and quantitative set of measurements and calculations for different colors, and your perception of color is at least as subjective.
I’ve studied pain, I practice medical pain management, and I collaborate with board certified pain management physicians. Pain is too broad and variable a subject with myriad various types and classifications of symptoms that are called ‘painful’ to ever be very objectified at all. Pain scales are really only useful in tracking a specific individual’s pain level, and even then the reports vary.
Easier to classify it by patient function level, frankly. Is their pain so debilitating that they can’t do their basic self care? An exercise routine? Household tasks? Their job? Again, very variable depending on the individual, but at least you can rank them. And since pain management treatment is focused on improving function rather than reducing pain, it’s a more useful measure.
I would think it falls under “technically possible but not useful”. For instance, measure nerve responses - how many nerves trigger or how often. Or, brain scan to see how much brain lights up in response to a stimulus. Not useful except maybe diagnosing nerve problems below the brain stem, because what everyone else said about subjective ness. But IANAExpert.
People experience pain with varying levels of stoicism and resistance. There are many types of pain - psychosomatic, neurogenic, musculoskeletal, referred, etc… and many causes. It is a very complex subject. In general, the more treatments that exist for something in medicine - the more complex and less effective any specific treatment and the less understood the subject.
Because pain involves a complex mix of inflammatory mediators and various chemical families it may well be possible to quantify these biochemicals. This may lead to a useful method of determining pain levels. Though I think in a hundred years such a test will exist, it may not change practice that much.
Our current understanding is far from that point. Doctors tend to believe the amount of pain a patient claims; unless there are reasons that make this less likely. This is an unsatisfactory situation for everyone as it leads to pain often being either under treated or over treated and both of these cause other problems.
At the moment, though, even if there was a test that somehow came up with an accurate number individual variation would probably make it of limited use in practice. It would provide a starting point and need titration, but this is what already exists.
One would guess that if it were possible to quantitatively measure pain receptor output a more objective measure might be possible. But we know that there is variation in sensitivity of receptors as well. But this might be calibrated. A PET scan might provide some clue. But working out a baseline activity would be impossible for someone already in pain. A fMRI might work.
The usual 10 = worst pain imaginable is clearly highly variable, subjective and modified by experience. A friend of mine suffered a perforated colon due to a mistake in an earlier surgery. By the time she was carted to emergency some days later her BF was worried she would die from the pain, she was so wracked with pain. If that is a 10 I doubt I have ever got to a 7 and hope not to.
I would imagine that paramedics get to see an extreme range from squeaky wheel hypochondria to arbitrary trauma. How fast they reach for the Fentanyl must require some interesting judgment.
You could do exactly the same with pain but you’d have to subject every person to different levels of pain in order to calibrate their pain scale. It works with colour because most people experience colour every day and a lot of their early years focusses on coming to an agreement with other people as to what each colour is called. This calibrates our colour scale so that when I say “red” you know that I’m talking about a range of colours similar to what you think of as “red”.
So you’d need to spend time with babies and toddlers, sticking a knife in their stomach, breaking bones, burning their hands etc and saying things like “No Timmy, the knife in the stomach is a 7, not a 10, you will understand better when we pull your finger nails off.”
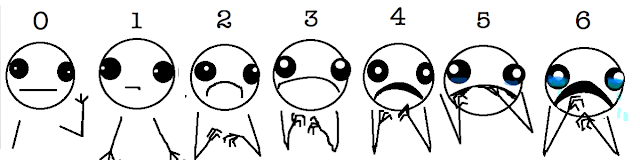
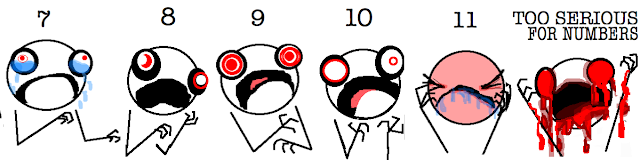
No doubt everyone here is familiar with the new illustrated pain scale from hyperbole-and-a-half, with pictures that look like something from Fear and Loathing in Las Vegas :
In fact, there have been attempts to quantify pain objectively. Yes, by actually inflicting pain on subjects and measuring (somehow) their responses.
There was an attempt to define a measurement of pain, in units called dol (from dolor). I read a book about it once, but I’ve never heard of it since. I guess it never really got traction.
The dol scale I read about (may or may not be the one described in the article linked above) was a logarithmic scale, like the Richter scale for earthquake magnitudes. It ranged from 1 to 10, but with a few pain sources rated above 10 or “off the scale”. I think serious burn was one of those, and another was the sting of a stingray.
There was an article just a day or so ago about a woman who jumped into one of those boiling-hot Yellowstone pools to save her dog, and ended up in critical condition with severe burns from her shoulders to her toes. That’s probably up there on the scale. (Spoiler: The dog died.)
Okay, here’s another brief note I found: Some scientists in the 1950’s subjected subjects to increasing levels of heat, seeking to determine the “just noticeable difference” in heat. (I can see a problem with this already – think about boiling frogs slow vs fast.) A dol was defined as “two just noticeable differences”.
You also have to factor in that our society tends to place greater value on people who claim not to experience much pain and lesser value on those who claim they do experience more pain. Is the patient truly experiencing only a “4” with all those glass shards sticking out of his face, or is he experiencing a 10 but worried he’ll sound like a wimp?
There is more to diagnosis than pain relief.
Understanding the problem extent nature and intensity is going to inform further efforts. Modern medicine has yet to reach the stage where a bunch of scans and lab tests yields an answer. Proper doctoring involves a lot of reading of the patient.
When I was in college, I became friends with a researcher who oversaw clinical studies using human volunteers. I did it for the money, not out of altruism, so I’d look for offers with big payouts and minimal discomfort. Sleep studies paid well.
I did a study once looking at thirst, measuring different parameters while the patient was made more and more dehydrated. Thought it would be easy, hell thirst is no big deal, right? I was hospitalized overnight, kept off fluids, then given concentrated saline IV to gradually make me very dehydrated.
I had to rate my thirst 0-5 IIRC. I remember quickly running out of numbers and having to recalibrate. Ever watch a western movie where the hero is trudging across a desert in the sun, their face parched and their lips swollen? I was that guy.
To objectively quantify? As in the thread title? Or to more objectively measure, as in the closing sentence?
It’s obviously possible to improve the objectivity. And you don’t necessarily have to deliberately cause pain to do it. You could study categories of injuries and the number scale answers people give in emergency rooms, with millions of data points, and study the statistics. You could opportunistically monitor things that were painful but predictable and necessary, like vaccinations or medical procedures. And of course you could include numerical signals like changes in vital signs.
You could get volunteers to be hurt, for some amount of money, with the bidding process taken as an indicator – how high will they go? They’d lose the chance if they held out too long, like in an auction. I’m not sure how this works ethically, because they only get hurt when they offer to get hurt, and you’d have to have some way to account for the significance of the money to each subject, as billionaires and people in debt crisis are going to have different motivations.
You could create a ranking scale, which is certainly quantitative even if it has no units, and is I think more objective than the smiley frowney spectrum. Would you rather hit your thumb with a hammer, or have a filling done without anesthetic? People can only answer for pairs of experiences they have had.
In a lot of these, the strength of the improvement in objectivity comes from the statistics. After all, musical tastes vary all over the place, and yet there are lots of objective and quantitative measures of the popularities of musicians.