When someone says the artery was “50% blocked” do they mean the inside diameter was decreased by 50% or the area of the open cross section was decreased by 50%?
The best measurement appears to involve determining the degree to which blood flow is impaired.
As you note, there are some complexities to the question.
In my experience, this is generally reported as maximal diameter stenosis. That is, the worst degree of narrowing in one projection. There are some theoretical advantages to using area stenosis, but in practice this is more difficult to measure, and any difference is probably not that relevant.
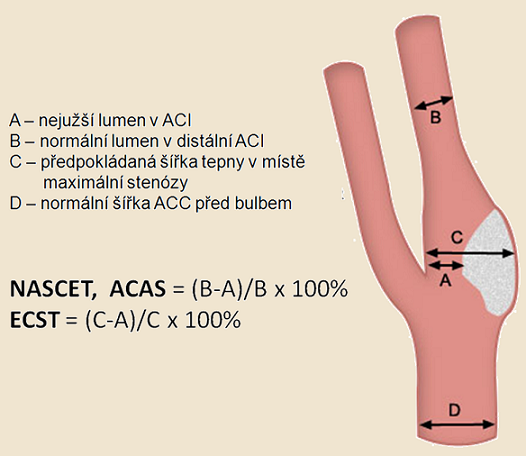
The carotid artery is particularly tricky, as the region most commonly affected by stenosis (the carotid bulb) is naturally a bit larger than the rest of the vessel in normal people. Some measurement schemes call for imagining the natural contour and then using this as the denominator to calculate diameter stenos. The standard in the US is to use measurement as defined by the NASCET trial, which is to compare diameter of the stenosis to the caliber of the normal distal vessel.
Many people “eyeball” the vessel (however it was imaged) and guesstimate the stenosis. This has the advantage of tending to upgrade the stenosis (that is advantage if you want an excuse to treat). In my experience, the stenosis always looks tighter by “eyeball” than by measurement.
Lastly, Doppler is often used, and relies on velocity acceleration through the stenosis. Various studies have associated different measurements with different degrees of diameter stenosis on angiograms. Doppler results are merely a proxy for angiographic results, and should not be expected to perfectly align.
Interestingly, the physics of blood flow velocity imply that Doppler comes closer to measuring area stenosis than conventionally performed angiography.
Here are some pics
Here’s a slide that disagrees with my eyeball claim- looks just as good as measuring here.
All I can say is that I have seen overestimation of stenosis by eyeball over and over, by my own and others.
Here’s a paper that supports the notion that diameter stenosis correlates reasonably with area stenosis.
Interesting. I ask because I recently had angioplasty on my mid cerebral artery. As I understand it, an initial angiogram indicated a 70% blockage. Apparently, this was revised to 80% at some point (during the subsequent angioplasty?) because that’s the figure I saw in my records. Medication was tried but transient stroke-like symptoms were becoming more frequent. The angioplasty was determined to be the best course of action. There were some complications and it was necessary that a stent be placed. Anyway, when all was said and done they said that the blockage was now down to 50% and that’s what they were shooting for. And, apparently, it wasn’t plaque as there is no evidence of plaque or stenosis anywhere else. I never thought to ask what this % number meant, assuming that it was the interior diameter. It wasn’t until after I got home and started thinking about it that I realized that a 50% reduction diameter as opposed to a 50% decrease blood flow are very different things. (I prefer the blood flow but I don’t get a choice). I never even considered what BBB’s link points out - the artery is getting narrower downstream anyway so the stenosis being compared to what? In the U.S. I guess its being compared to what it should be at that particular place. Diameter or blood flow question aside, its pretty amazing that the body can function relatively normally with a 50% reduction. I’ll have to ask about the numbers when I go in for a follow-up in a few months.
Middle cerebral artery or internal carotid artery?
I ask because treatment of ICA stenosis is common, but treatment of MCA stenosis is decidedly uncommon (but happening more nowadays as the technology advances).
Since this is about an actual medical condition, let’s move it to IMHO.
Colibri
General Questions Moderator
Mid cerebral, for sure. The neurology docs were kind of excited about it because they rarely see it. From what they tell me, I was the talk of the department and consults were ongoing with docs at another hospital. I was to a topic at “grand rounds”, whatever that means. Kind of a mixed blessing I guess. I mean, who wants to be the topic of such conversations? On the other hand, having lots of input from people at one of the top hospitals in the Philadelphia area can’t hurt. I have lots more questions regarding blood pressure, the circulatory system, strokes, etc if you’d care to entertain them. They can wait until my next appointment but, while related to my condition, they are bit more general in nature and time is at a premium during office visits.