Mrs. Charming and Rested has a cough and cold symptoms (including fever under 101 degrees at its peak) that have persisted for about nine days. Two other people seemingly infected at the same time and presumably from the same thing (me included) largely recovered in the last day or so. Several home tests over several days for both of us are negative for COVID. Mrs. Charming and Rested had a tele-health appointment, was diagnosed with bronchitis, and prescribed antibiotics. How does a doctor know based on this information whether antibiotics are appropriate or would be useful?
Bronchitis is an inflammatory condition of the bronchus (lower respiratory tract), not an disease in and of itself. Bronchitis can be caused by bacterial infection but in adults is more typically a result of a respiratory virus or a condition of chronic obstructive pulmonary disease (COPD). I don’t know how a doctor can determine a bacterial from a viral infection via a telehealth session because bacterial cause is usually determined by oropharynx swab and enzyme immunoassay. There is generally little treatment for respiratory viral infections other than palliative care and allowing the virus to take its course so it may be that the doctor just prescribed antibiotics as a precautionary measure, which is an unfortunately common if not recommended practice among general practitioners leading to antibiotic overuse.
Stranger
Well, she doesn’t have COPD or any other pre-existing health conditions. I recognize that antibiotics aren’t useful for viruses. I’m curious if any doctors or NPs think the prescription was a good idea.
With a fever and symptoms lasting 9 days, are you sure the diagnosis wasn’t pneumonia?
~Max, not a doc
It was not. The fever didn’t last nine days. I believe it lasted one or two.
Not a doctor, but I had this exact same question for a doctor, in almost an identical situation with a family member. Answer was basically this:
- Bronchitis is sometimes caused by bacteria (but very rarely)
- Bronchitis can sometimes cause a secondary bacterial infection
- When it has not resolved in 10 days or so, there is a higher chance that it could be bacterial
The way it struck me is these prescriptions are rarely (maybe almost never) issued for a “confirmed” bacterial infection, I think they are just commonly given for bronchitis that persists longer than a certain period of time, because there has been a decision made that in such cases, risks have gone up for it being bacterial.
Purely my opinion but I got a bit of the impression of it being a thing where doctors view it as “well at this point it could be worth using, and it doesn’t hurt really to use antibiotics.” I don’t think it is normal at all for them to do it with bronchitis that has only been short lived, in my family members case they had had it for over two weeks.
Based solely on the info presented in the OP, I would not be prescribing antibiotics in that situation. Antibiotics are horribly overprescribed, especially for respiratory symptoms. And such overprescription can cause harm by causing resistance.
Thanks Qadgop_the_Mercotan. This is my concern too. I was hoping to learn that this was a good idea and my wife was being well-taken care of but I appreciate knowing my worry is not unfounded.
Antibiotics also wreck havoc on the gut microbiome and can cause adverse immune response and inflammation. Quality controlled pharmaceutical-grade antibiotics are one of the great innovations of modern medicine, saving many millions of lives and treating infections that might otherwise result in amputation or debilitating chronic injuries, but their use should be targeted to specific bacterial and fungal infections instead of being applied willy-nilly. “Prophylactic” use of antibiotics is like applying chemotherapy to treat a benign cyst and generally should be avoided except for patients who are vulnerable by a pre-existing immune compromised condition.
Stranger
Also inappropriate prescribing results in more; untoward allergic reactions, interactions with other medications, alterations in certain nutrient absorption, increase in photosensitivity, risk of autoimmune phenomena, and many other oft overlooked effects. Proper antibiotic stewardship by prescribing practitioners is absolutely necessary, but both public expectations and prescriber desire to please the patient run contrary to this principle all too often.
So what factors might lead you to prescribe antibiotics in a similar tele-health appointment for similar symptoms? Would you request lab work and prescribe only based on the results? If the symptoms had persisted for a while, might there come a time when you would prescribe antibiotics even without labs? What if the coughing were reportedly getting worse (which isn’t the case for Mrs. Charming and Rested)?
And what do you think about Martin_Hyde’s conversation with a doctor who suggested that maybe a longer term infection would suggest that it is bacterial. What are the odds?
Cough over 3 weeks would make me take a closer look, but even then antibiotics would be considered only if there were appropriate findings such as parenchymal infectious disease or COPD complicated by purulent sputum, or immunosuppression.
Here’s the starting algorithm for cases such as you describe, from UpToDate
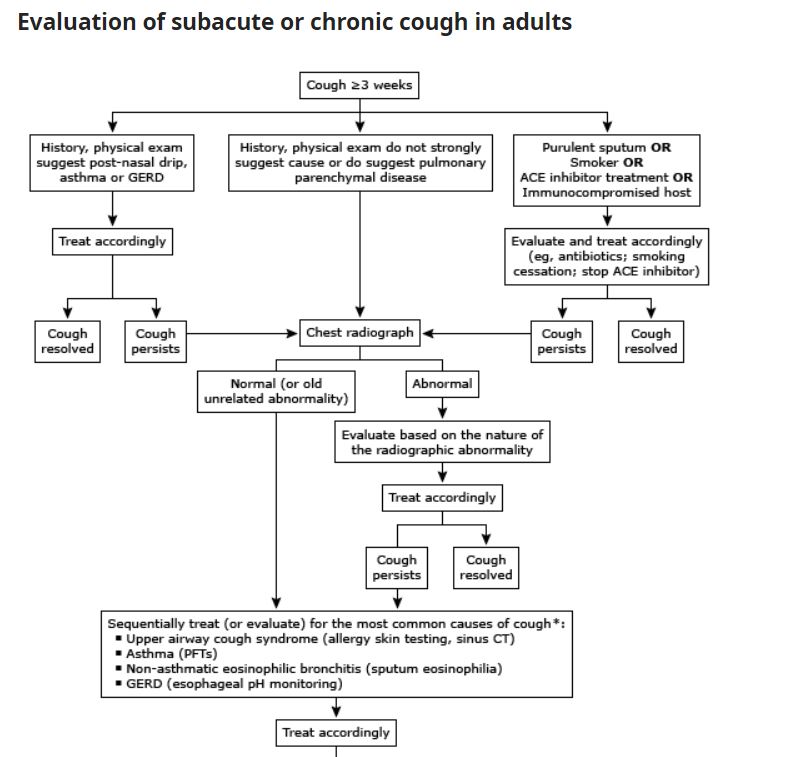{kind=link}
Thanks again. Her coughing has been going on less than three weeks. She may have post-nasal drip (which would explain some of her throat irritation). She definitely has some congestion but she doesn’t have purulent sputum as I understand the term. The treatment according to the chart is “treat accordingly” without specifically mentioning antibiotics.
Exactly. Antibiotics would be employed only for presumptive diagnosis of cough caused by bacterial infections. Most coughs are NOT causes by bacterial infections. So if the diagnosis is cough due to ACE inhibitor use, stop the ACE. If it’s due to reactive airway disease, treat that. Etc.
Not (!!!) a doctor, but I have a huge tendency to post-viral bronchitis, and sadly, it tends to be self-reinforcing.
So I get a horrible, consistent cough for days after a minor cold comes and goes. My PCP basically found it was self-reinforcing - I was coughing so much my throat would be raw and irritated, which prompted me to cough more, which … on and on and on.
I wasn’t showing any other symptoms or temps though. So the first 2-3 times they gave me antibiotics anyway for all the reasons posted above which basically did little to nothing. After that, they got wise, and prescribed me a steroid inhaler and/or in office vaporizer to fundamentally numb the affected area and break the cycle.
I cannot say (as I am NOT) a doctor, but it may be a similar issue for your better half, and something to explore if the antibiotics do nothing for her.
There are very few times that prescribing antibiotics via telehealth is good medicine (oh say two weeks of worsening runny nose and cough which hits the clinical definition of sinusitis, video visit and/or photos sent of what is clearly impetigo …) but telehealth is much more frequently a driver of excessive antibiotic use based on inadequate assessment. Prescribing is faster than explaining why it is not being done and talking through the what ifs.
The perception of the decision makers though is that this is what patients want and that a group will lose patient visits if they don’t play in the space. The faith that patients (or their parents in my case) understand what good care requires instead of just getting the meds is not there.
To the non medical here- are they right or wrong?
That was kind of a question I wanted to ask–while I often see doctors in contexts like this message board, private conversations etc bemoan overprescribing antibiotics, my experience (mostly managing health visits for elderly relatives) is most front-line physicians generally are fairly prescription-happy across the board, including on antibiotics. I actually remember an incident in which my sister wanted to be prescribed an antibiotic, because she perceived it as necessary, and her doctor told her no. She chewed his office out on the phone and then went to another doctor who immediately wrote her a prescription. I have to think someone running a GP office has to worry at least a little bit about angry “customers” deciding to go elsewhere, like my sister did.
As a parent, I will say that, sometimes, when you go to the doctor with your sick sick kid, you kind of just want a magic solution. When my son had RSV and wheezed for 6 weeks straight, we went to the doctor and the ER so many times only to be sent home after they verified that he wasn’t, at that moment, actively dying. It was heart wrenching. Though I was frustrated at the time, I realize now that the doctors couldn’t do more for him at the time. There’s no magic pill that will make your child better.
That said, when antibiotics ARE warranted, they are lifesaving.
The customer is always right, eh?
Well, those doctors seem compatible with Mrs. Charming and Rested, who seems pleased that the doctor is doing something to end her suffering. I, on the other hand, would question the need for antibiotics without reason to suspect a bacterial infection.
As a pet parent, I was recently very pleased when my vet said that an infection on my dog’s lip would clear on its own. In the end, when it took longer to clear up than he thought, the doctor recommended Neosporin, which worked. I wouldn’t have been happier with an oral antibiotic from the get-go that gave Cranky Dog diarrhea. It’s not a waste of my time for a doctor to reassure me that it’s going to be okay and it won’t become some agonizing horror show later.