Badly infected/inflamed cysts are very difficult to anesthetize by local, I testify from multiple personal experience.
I have never had a pilonidal cyst, but everyone I’ve ever know who had them described the same pain as the OP. So I’ll pass on them, thank you.
Regarding the pain scale: often the important part of it is to get a relative pain level and then learn later if the patient perceives there has been a change in either direction of how much pain is being experienced. The 1-10 scale is merely part of the entire picture. That being said, if you want to throw out a benchmark (“With 10 being that massive car accident I was in a couple years ago/childbirth/testicular torsion, I’ll give this a 7”) it probably could be useful.
Scales are rough. In college, I picked up extra cash as a test subject in medical experiments. One looked at dehydration. In a carefully controlled setting, I was dehydrated via IV hypertonic saline.
I had to rate how dehydrated I felt on a 1 - 5 scale. I quickly reached 5 and had to adjust as things worsened. Repeatedly. (Paid well, though)
Well, because not all ailments are painful. If your hair started falling out in clumps, you’d go see a doctor even if it was painless, wouldn’t you?
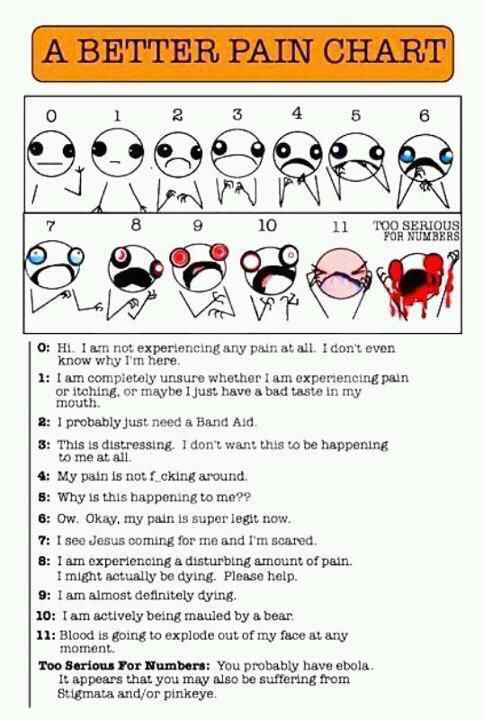
I think this scale works nicely. In fact, I think it should be official.
{kind=link}
Ha! I once had a pediatric dentist tell my mother I was a brat when I cried during an extraction. It was an abscessed tooth – I lost the filling and since it was a baby tooth, they just pulled it out. She didn’t use enough novocaine, and it hurt like hell. I cried, of course – plus it sucked that the mirror WAS RIGHT OVER TOP OF ME, so I could see what they were doing. Then she complained to my mother that I whined about it. Bitch.
The next time I had a baby tooth out – the root was too long to fall out on its own – she shot me up with so much novocaine I couldn’t even taste anything for hours. Oh well.
(My dentist now is great. He is the nicest doctor ever)
A better scale
From a source frequently referenced on SDMB.
Patients do exaggerate symptoms, but most of the time it doesn’t make any difference to the treatment. I give antibiotics for upper respiratory infections based on whether there are objective signs of a bacterial process or not, not how bad your sniffles are.
The problem comes when patients who either really do have horrible cold symptoms or who say they do feel like you’re belittling them by recommending fluids and OTC meds, as if you’re not taking them seriously. Some docs make it worse by saying it’s “just a cold”. What you have to do is acknowledge the symptoms and their severity, empathize a little bit, and explain why you wish an antibiotic would help but it won’t.
Even then you’ll have plenty of people coming back the next day to see the nurse practitioner to get $80 worth of antibiotics, or complaining to the CEO of the clinic that you didn’t do anything for him. But all you can do is all you can do.
That was a tangent. But the bottom line is that a given set of symptoms generally calls for a given workup and/or treatment, so playing the severity of the symptoms up or down doesn’t really change what you do very much, even if it might change how you present it.
Backgroud: I had unearthed some old books from storage and tucked them into my headboard for my re-reading pleasure.
A series of bumps appeared on my forehead, and I thought maybe a couple of spiders had hitched a ride with the old books.
I gave the spider bite story to the doctor, who was looking at my records while I explained everything. He took one look at the bumps and said, “Have you ever had shingles?”
No spider bites for me! He checked to make sure my eye had no lesions, and I ended up looking like a Romulan halfbreed for a couple of weeks.
~VOW
I live in the land of Generous Motors insurance and have quite a few friends who have awesome health insurance. And I can think right now, off the top of my head, of three (more, actually) who take themselves or their children to the doctor at the slightest hint of congestion or common cold symptoms or paper cuts or any unpleasantness that lasts for more than a few hours…
And who are insistent that the doctor give them “something” to relieve the wittle discomfort they or their brood are experiencing, and who will complain mightily, then go to a second doctor or clinic, if they’re not given PILLS FOR SOMETHING, RIGHT NOW.
We’ve had conversations about this. But it seems that there are people who feel entitled to a prescription whenever they go to the doctor, and feel as if they got inadequate treatment if they don’t walk away with at very least, a scrip, and preferably CT scans and MRI’s and blood work and x-rays. For a cold.
Not terribly relevant to the OP, but funny with regards to you story: I once went to an MD with a weird lesion he diagnosed as a spider bite. Saw a dermatologist the next day for something else, and he asked me about my shingles. Turns out he was right.
Yes, exactly. It’s *supposed *to be subjective. I want to know if this treatment is working to ease your pain, and since we forget about pain intensity rather quickly (like labor pain), putting a number on it now and a number on it after [massage/heat/ice/meds kick in] helps us both know whether or not to do that thing again, or if we need to try something else.
Also, it gives us a way to set a realistic goal and see if we’re all on the same page here. If a person comes to me with pain at an eleventy four and three herniated discs and shingles and they say that they want their pain to be at a zero, I know we have some educatin’ to do. Ain’t no way, bub. But let’s consider if you can get through the day with a 2, okay?
There’s no right answer. There’s no number at which I’ll necessarily give you “the good drugs” when I wouldn’t at a lower number. There’s no number at which I’ll ignore your pain as unimportant if it’s important to you (and lowering it is realistic with modern medical techniques.) It’s just a way - and only one way - that I can tell if I’m doing my job well and which treatments are most effective for you.
My husband encourages me to do this, and I’ve done it on occasion. He says I have a whacked pain scale.
When describing symptoms to a doctor, I try to take the witness stand approach - facts only, and answer the question that is asked. If I feel the need to editorialize or speculate or characterize, I try to frame the statement using the words “I’m editorializing here…”, or “I’m speculating here…”, etc.
I find that it is really difficult for most humans to talk using facts and data without opining or elaborating, so I try to do my part in these situations.
Each doctor I’ve seen has a different way of assessing me as a patient.
I had one doctor who would drive me CRAZY. I’d come in half dead from bronchitis or sinus infection and say something like, “I feel like there’s an elephant sitting on my chest,” or “I feel like I was just run over by a Mack truck.” His response would be, “But how does that FEEL?”
One of my favorite encounters was because of a bladder infection. The doctor took one look at the lab results and said, “You’ve had this before, well, you’ve got it again.”
IMHO, a truly responsive physician will also listen to the little, almost inconsequential symptoms. I took my son in when he was four months old. The kid was a champion baby: ate and slept with no problems. He had been sick with a fever, and my chief complaint was, “He won’t sleep.” Now, when my daughter was an infant, she didn’t sleep for the first year of her LIFE. My son, hey, I put him down at 7 PM, and wouldn’t get a peep from him until the 2 AM feeding, and then after being fed and changed, he’d go right back to slumber. With the fever, as soon as the Tylenol wore off, he’d be awake and crying.
So it was a very minor symptom.
He ended up being admitted for possible meningitis.
Several years ago, I didn’t know what was wrong with me. I was constantly upset, crying, couldn’t focus, couldn’t work. I wanted to curl up like a pillbug and just shut out the world. My husband DRAGGED me to the doctor.
My complaint? I felt like something TERRIBLE was going to happen.
My mother had died about six months before. My father had just informed the family he had prostate cancer. I was losing my marbles. My doctor gave me a prescription for an antidepressant, and a referral to a counselor. While I sat sobbing on her exam table, she put her arm around me and said, “Everything will be okay, I promise.”
~VOW
I try to give my patients some perspective about the pain scale. It is subjective, but it needn’t be completely open-ended.
I tell them “on a scale of 1 to 10, with 1 being pain you really have to think about to even notice, and 10 being pain so bad you’re tearing the skin off your arms with your teeth to distract yourself from it, how’s your pain right now? How bad does it get at its worst?”.
If the patient declares the pain to be a ‘9’ while he’s sitting there comfortably and relaxed, I thus make allowances for that. If he’s rocking back and forth, sweating and grimacing and says it’s a ‘3’, that has its own meaning.
And I have no idea how much different medical services services are worth, as I’m paid by the hour, not by the patient. And my patients don’t have to pay for their procedures, other than the occasional $7.50 co-pay. If I have to start giving private practice fee and pricing information as a condition of providing medical knowledge here, I’ll have to stop dispensing knowledge. :rolleyes:
Speaking of trick Q’s - was this a trick, or are these people too dumb to be given stethoscopes?
I have stage IV CKD.
I also have Osteoarthritis in both shoulders, and elbows. My lumbar region looks like a question mark.
A few months ago, I peaked my Creatinine from 1.98 to 3.22 - which got me to the front of the line to see a nephrologist.
I was asked "how are the (NSAID’s) working? They won’t give me credit for knowing NSAID - so they say something like “Tylenol or drugs like that”.
In front of them is my script list. MS Contin and hydromorphone.
Do they really think I’m ignoring these and using NSAIDs?S
Why on earth did she ask that idiot Q.
That was the RN in receiving. I got it again from a senior nephrologist in the exam room.
Anyone care to spill the beans on their fellow physicians?
I also have a very high IQ, and have been seeing my PCP (all of these folks work work for UCD) long enough that see knows this.
Not a doc, but my WAG is that they’re seeing if you’re taking NSAIDs in addition to the other meds on your list. Plenty of people will take certain medications, especially OTCs, but not write them down, like they don’t “count” or something.
I work in ophthalmology and do similar “tricks” when asking patients about their medication dosage/frequency. I’ll be looking at their chart showing what they were told to take at the end of the last visit and will ask “so how many times per day are you taking that drop? and which eye?” If I just say “and are you taking the Timoptic 3 times a day in your right eye?” I’ll get agreement. If I ask what eye and how often, then there will be plenty of times where I’ll hear they’re taking it in both eyes rather than one/one eye instead of both/wrong number of times per day. For some reason, prescription eyedrops are often treated like “doesn’t count” meds.
In 10 months of nursing, with probably 300 patients in that time …I had exactly ONE who gave me their drops, inhalers, topicals (ointments/salves/creams), patches, or supplements when asked to “gather all your medications, including anything you buy without a prescription so I can get a list of everything you take or use for your health.”
In the last 3 months, I’ve learned to be more specific: “…don’t forget your inhalers or creams or herbs and supplements!” …And I still don’t get vitamins or whatever they take to make a headache go away until I ask them again when I see them.
If it doesn’t come in an orange plastic bottle from the pharmacist, it doesn’t count, apparently.
But you’ve started asking specific questions. Last time a surgeon’s nurse asked what meds I take, I did not understand the nurse wanted to know about fish-oil. But last time I gave blood and the nurse asked about meds, the nurse couldn’t have cared less about fish oil.
Specific questions are good. I don’t understand what is relevant information in different situations.
It also may be because the use of NSAIDs in the context of chronic kidney disease would be very important to know about. And guess what? Lots of people on MS Contin and hydromorphone add in an NSAID when they don’t do the trick. And most won’t mention them as meds they are taking unless asked explicitly, and even then some know they are not supposed to and won’t answer yes the first time it is asked.
Actually they’d be negligent if they did not do that. They are not insulting your intelligence; they are doing their job.
The vast majority of pain scale questions I ask are answered “7.” Almost always “7.” For my uses (kids) I like to find out if it stops activity and impacts function. Can they play through it? Do they have to lay down? (For history over things like headaches.) How do they get on and off the exam table? (For acute pain like belly pain.)
“Lethargic” always needs more … “What does lethargic mean to you?” Often they just mean tired or wanting to lay in a parent’s lap and watch TV, but it can mean very seriously ill out of it. Not making eye contact staring off into space lethargic? In peds we do a lot of assessment over the phone on call. Is this a kid who needs to be sent to the ED? Seen tomorrow? Reassured? Figuring out which story is being under or oversold is critical stuff.