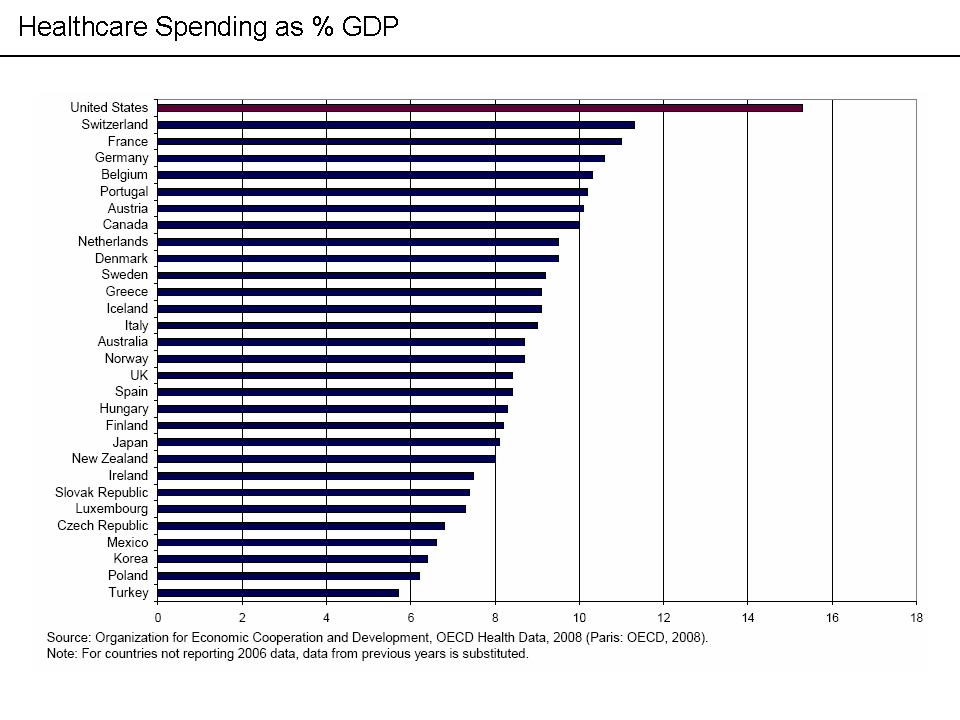
America spends about 16% of GDP on healthcare, as opposed to 8-11% that virtually all other wealthy countries spend.
Health care systems have different setups. Public payer, public provider (NHS in the UK, US VA system), Public payer, private provider (Canadian Medicare, US Medicare). Private payer, private provider (Netherlands, US health insurance). In and of itself, public vs private payer or provider does not seem like the big cause of health care costs.
Switching to a ‘medicare for all’ system would save $400-592 billion a year. Figures vary wildly, the largest I’ve seen is $592. The lowest is closer to $300 billion.
However we have a 17 trillion economy and spend $2.8 trillion on health care. Even if we cut $400 billion a year in health care by adopting single payer, that will only shave our health expenses by 1.5% of GDP. We will go from having far and away the most expensive health system on earth to far and away the most expensive health system on earth. If our system were as efficient as Israels we would spend 1.36 trillion a year on health care, not 2.8 trillion.
Israel has a multi payer system, not single payer. They spend 8% of GDP on health care. France has a multi payer system, was recently found to have the best system on earth and spends about 12% of GDP.
Even PNHP, a physician group that advocates for single payer, admits that single payer will not solve the US’s health care system woes. The real problem is how our health care system is run and structured. It is fragmented, doesn’t use public or private market forces (negotiations, transparent pricing, comparative effectiveness, etc) and is incentivized to provide the most expensive treatments possible.
The payer is not the problem (public vs private). Many OECD nations have private payer systems and their costs are in line with nations that use public payer systems. The real problem is how our health care system is administered and run (or not). There aren’t enough incentives to cut medical costs, and too many incentives to drive them up.
I don’t know the solution, I’m sure people far smarter than me have figured it out. But evenso, I seriously doubt the actions necessary to change it will happen anytime soon. Maybe on the state level, maybe. But the federal level seems like a lost cause for the next decade or so.
Even if a state tried to impose cost discipline on health care systems, would that really work or would health care providers pull up shop and move to another state?
{kind=link}