Yes Broomstick I did mean all extended family that is alive that might share the gene. The difficulty to get screening surprises me. Screening questions looking for risk of those conditions (including drownings that may have actually been dysrhythmias that occurred while swimming) are part of sports clearance exams which trigger that evaluation.
Sorry Shodan for using the abbreviations. I hope the links already given answered the question.
It shouldn’t - the medical industry is under significant pressure to keep costs down and there are frequent demands to justify things that should be granted automatically. Because someone with the gene I mentioned may not show symptoms until well into adulthood insurance companies are really reluctant to pay for screening. Even when they do pay for screenings individual doctors may be reluctant - my niece’s doc didn’t want to schedule her for an echocardiogram because he didn’t see a reason for it, seeing no overt signs of heart disease. It took a phone call from my-sister-the-doctor (her mother) to get this done, and that was AFTER a genetic test showed that the niece had the gene. If my sister had not had an MD after her name I don’t think the other doc would have given her the time of day.
(Slight diversion: when my sister questioned one of the docto’s involved with my husband’s final illness he got all huffy and asked the loaded question “Oh? And what medical school did YOU go to?” Wish I had had a camera for his expression when she told him her medical education in detail as well as current job. Yep, assumptions can get you in trouble…)
That is how life is for the majority of Americans. Getting screening can be a bitch. Getting preventive care outside of currently legislated mandates can be a bitch.
Remarkably enough, I don’t think any of my relatives have ever drowned. Nevermind how much time we all spent swimming. We did have a lot of early deaths in the family. My generation did sports before modern screening for that sort of problem. Not sure about the following generation - all of the nephews and the niece got through high school sports screenings with no signs of trouble, which I’m told is not unusual with this particular genetic issue. I don’t personally understand the details, but I’m told that unless you are looking specifically for this disorder you are unlikely to ever find it. My sister-the-doctor has tried to explain it to me, but without a great deal of success in part because this is a very emotional topic for her, what with her own 30 year battle with what we now recognize is this syndrome and with passing it on to her children. I don’t really want to ask her about it again.
I’ve been in practice within the medical industry for over three decades. Never ever a demand to justify for a screening EKG or echo. Not once. We take care of patients with all sorts of plans too. They are just not high enough cost items to warrant it. MRIs sure (and for this specific rare familial cardiomyopathy it seems that a cardiac MRI and Holter might sometimes be needed to find it), certain expensive genetic tests, yes, some medications, yeah. Not once for a screening EKG or echo. Mind you I’d question someone ordering them on every patient as a matter of routine (and there are some who advocate screening every teen with an EKG).
My own experience is that we are under great pressure to prove we provide measurable quality and value. Not blindly limit cost.
Individual providers not understanding the significance of the family history? Sure that can happen. Shouldn’t but does.
A routine sports physical would not pick this up. It would though have the family history raise the flag to minimally get the EKG and echo and with that strong of a history of sudden death at early age, be it cardiac or drowning or unexplained but especially if during sports, maybe straight to pediatric cardiology.
I gather the deaths are not recent but my condolences for your family’s losses. Death of a child is always a very hard grief and the grief your sister experiences may be especially … complicated.
Your father had no siblings? No cousins who should know about the possible risk?
He had a brother who died at age 30. Attributed at the time to a sudden heart attack.
There are some garbled/uncertain tales of young death in prior generations, but the 19th Century was full of ways to die young.
No, the family was almost completely killed off in WWII.
Dad’s brother produced one child. We know she is deceased, but not her cause of death. We did not get along with her and the last contact any of us had with her was the early 1980’s. She had no children of her own.
Broomstick, my condolences for your loss. I just wanted to say that my snark about “who is this ‘you’ that you speak of?” was not at all intended as defensive of my particular situation or any perception that you were criticizing it. It’s just that it seemed to me that the ambiguity about whether “you” referred to the doctor or the patient in that observation invited comment, namely the comment that it should be an informed consensus of both, a very important point that I wanted to emphasize. It’s a point that ISTM the medical profession often neglects, especially in elderly patients, who are sometimes treated as if they no longer have the ability to make meaningful choices. Medical defaults can sometimes be cruel, such as unnecessary and sometimes painful medical testing when there would be no practical treatment in the event of a positive result anyway, or worse, the kinds of desperate lifesaving measures that DNRs are explicitly intended to protect against.
Anyway, on the matter of PCI/stenting, I wasn’t able to find the paper(s) I was originally looking at that suggested that techniques like FFR were bringing PCI into the same survival rates as bypass surgery, but here’s a recent paper that some might find to be of interest. It seems to depend a great deal on the specific nature of the heart disease (in particular, how many vessels are affected, and where the lesions are located) but it reflects the broad evidence that, while the debate is indeed controversial, in general bypass surgery tends to have fewer adverse recurrences than PCI, where “adverse recurrence” is generally defined as a combination of death, non-fatal heart attack, or the need for urgent revascularization. Nevertheless, the differences tend to be relatively small percentages, and could be skewed by other factors.
OTOH, if comparing PCI with medical treatment alone, the evidence in favor of PCI is strong. There was a clinical trial called FAME which sought to establish whether FFR-guided PCI was more effective than conventional angiography-guided PCI, and the answer was in the affirmative. There was then a second clinical trial called FAME 2 which sought to establish whether FFR-guided PCI was more effective than medical treatment alone. The results were so compellingly in the affirmative early on that the trial was stopped, on the basis that the patients being randomly assigned to the “medical treatment alone” group were being needlessly put at risk. More info on the various clinical trials here.
FWIW,i I will tell my story. Heart attack at age 28 in 1965. In 1972, I had a bout of galloping angina for which I was prescribed beta-blockers and nitroglycerin with a few weeks of bed rest. At this point I started walking 4 miles to me office 4 times a week (unless the temperature was below -20C (-5F) or there was a serious blizzard. I had an uncle who taught biochem at a medical school and he discussed this with medical colleagues. They were horrified that I had not had a bypass and attributed that to parsimony on the part of the Canadian medical system and maintained that it would have been automatic in the US. This was 1972, when the procedure was fairly new. At any rate, I have never had a bypass, although 12 years ago I had to stop the beta blockers and have a pacemaker installed because my heart rate was now in the low 30s. And I am still ticking, albeit with help.
I have known 4 people who had bypasses. Two them worked very well and they are still alive, one of the two is now 87 and had his bypass maybe 20 years ago. The other is probably around 70. There were problems with the other two. The first was neighbor and a McGill professor. They had trouble restarting his heart and he ended up with some brain damage. This seriously interfered with his profession and he was eventually retired on disability. This happened maybe 35 years ago and he died last winter in his mid or late 80s. The other one was a friend and collaborator, coauthor on a couple of my best papers. He was about 55 when had a bypass in 1990. Although there was no obvious brain damage, his personality changed and he became quite hostile to me. He stopped doing mathematics and his daughter had him put into a nursing home, although I don’t know the details. He died in 2006 never having really recovered.
Of course, this all has nothing to with stents v. bypass, but it does illustrate that it may sometimes be better to medicate than operator.
Er… no. My mother had her first bypass operation in the 1970’s, a bit later than 1972. Automatic? I think she got it largely because we were living in a large urban area with an available surgeon and team, plenty of places in the US you didn’t have that option because there weren’t an adequate number of surgeons and they were not evenly distributed across the US. She was put on a six-month waiting list, but she got her surgery in four because of the number of people ahead of her on the list who died before the surgeon got to them. Complication and fatality rates were significantly higher back then.
In sum: if you could safely avoid such surgery in the 1970’s and use another option that really was a good choice. Arguably, that’s not an unreasonable approach to use today.
My husband’s bridge partner had a multiple bypass and never really recovered his intellect. But he went in for surgery because of a massive heart attack, and I have assumed the brain damage (not an official diagnosis, just something evident to his friends) was due to the heart attack itself, not the treatment.
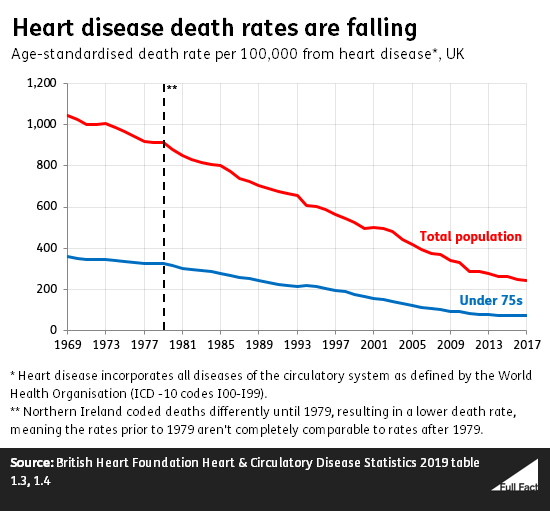
Which is great, but personally I don’t know how much is due to advances in medicine vs advances in public health.
There are many advances in medicine, and lots of people are being treated now vs in the past. Things like statins didn’t even exist until the 80s.
But I have heard a good part of the decline in heart disease rates is also due to declines in smoking rates. Then again obesity rates have risen which I’m sure is increasing rates too.
Regarding FAME and FAME2 (NEJM, 2012), it should be noted that these were trials looking at FFR guided PCI vs just visually (usually >70% stenosis). The biggest driver of the outcomes was the need for additional revascularization, not reduced MACE (major adverse cardiac events) or death, which are usually considered the more “hard” outcomes. It sort of makes sense as well. If you are undergoing a cath and afterward the interventionalist tells you that you had several areas that looked pretty tight but didn’t meet FFR positive levels, you might be a bit more sensitive to anything possibly cardiac related, driving an additional cath with PCI at a later date. ORBITA (noted above by myself) was pretty significant because it was a fairly well done trial in that they even did sham caths thus truly blinding the patient to which group they were in.
Deciding the superiority of the 3 possible arms (surgical bypass, PCI, or medical management) is a tough question because the indication for any procedure is always a question. In addition, medical management isn’t really an alternative; I would hope that any cardiologist worth the name would continue to treat with appropriate medications whatever the ultimate decision is. If you are having an ST elevation MI (the one usually portrayed on TV), then urgent revascularization is life saving treatment, whether it’s with clot busting drugs, PCI, bypass surgery, or some combination of all of the above. If you have stable angina, or chest pain that is reliably induced by exertion or stress and doesn’t occur at rest, then you’re most likely best off with trying to maximize medical/non-invasive therapies than jumping straight to PCI or surgery. Risk of cath are relatively low, but I’ve had people have strokes, suffer renal failure, or even die, and even knowing it was the right thing to do doesn’t make it any easier to have to explain afterward.
The screening for congenital heart diseases or arrhythmias is an interesting topic and I’m not weighing in too much other than to add that in some countries all children are screened with an EKG. The US had looked into this and felt that the false positive rate was too high to justify a universal screening, but like DSeid said, there’s essentially zero push back on ordering EKGs or echos. There is certainly push back on genetic counseling and all the things that go with that, but that’s a different story.
“CABG brain” has been studied fairly extensively, especially for people who have undergone valve replacements since those tend to have lengthy aortic cross clamp times. It’s a tough thing to pin down, though. Brain imaging may reveal new areas of infarcts but that may not lead to any actual cognitive defects. Transcatheter aortic valve replacement/implantation (TAVR/TAVI, two terms for the same thing) has looked at this quite a bit since it involves usually placing a new expanding valve inside a very calcified and stiff old aortic valve. When the new valve opens up, it can literally crack open the calcified fissures of the old valve and you get little showering of calcifications that go up the aorta and then to the brain or the rest of the body. Stroke is a known risk for doing these procedures. It’s tough to quantify non-large strokes, however, because often people have such improved cardiac output from the new valve that they perk up and think and feel better. But we also know that if you scan all their brains you’re going to find all sorts of new microinfarcts, and what do you do with that if they say they feel great? Certainly people can and do have large strokes like what is portrayed on TV but the general subjective feeling of “not right” has hounded the medical community for decades and will likely continue to do so. It’s a problem with medication side effects, for reported patient allergies or adverse reactions, for changes after surgeries, or for countless other reasons, and it’s pretty impossible to concretely study due to the inherent subjectivity of it.
I’m glad this is being studied, because I had the impression that this guy was considered a “success”, since his heart has been okay since then (several years ago). But really, he lost a substantial fraction of his quality of life.
I mean, I assume he would had died without surgery, so I’m not saying anything was done wrong. (other than him gabbing on the phone to my husband instead of calling 911. He was so wishy-washy about it that when he finally got off the phone, I suggested to my husband that my husband call 911 on this guy’s behalf.) It just seemed like it was only a very partial success.
The opposite happened to my dad- he had severe PTSD from trauma during the Holocaust. That brain effect from going on bypass ended up blunting some of his traumatic and intrusive memories, causing a significant improvement in his mood and quality of life. Happy accident…
That is extraordinary. And supports the idea that a treatment which permanently erases some memories (like using marijuana) can be successful in PTSD cases - since we have thousands of people mentally affected by the last 17 years of war who still have 50-60 years of living to do.
Wow, have to update this thread with this breaking story. Neil Armstrong’s death in 2012 was apparently caused by the botched aftereffects of bypass surgery, for which the family received a $6 million settlement for wrongful death that was supposed to be kept secret. I first saw this on CNN but the NYT article has a bit more detail.
The NYT seems to be the source – an anonymous party mailed a lot of documents about it to them, and they were able to verify enough of them via public documents that they published the story.