Total combined CEO compensation for the health insurance industry is approximately 100 million dollars a year. If you multiply that number 200 times you get to 1% of the savings you need to accomplish.
We could also demand that blood tests be performed by unicorns but it doesn’t happen.
You’re making the common fallacy in defended our broken health care system; you’re comparing how the American system works in theory with how other systems work in reality. And in such a comparison, the American system wins.
But with the American system in reality, plenty of people don’t get their choice of doctors or short wait times or the best care. And they don’t get the health care they’d get in Canada either. A lot of Americans simply don’t get health care. And a lot more get only the minimal amount of health care they can afford.
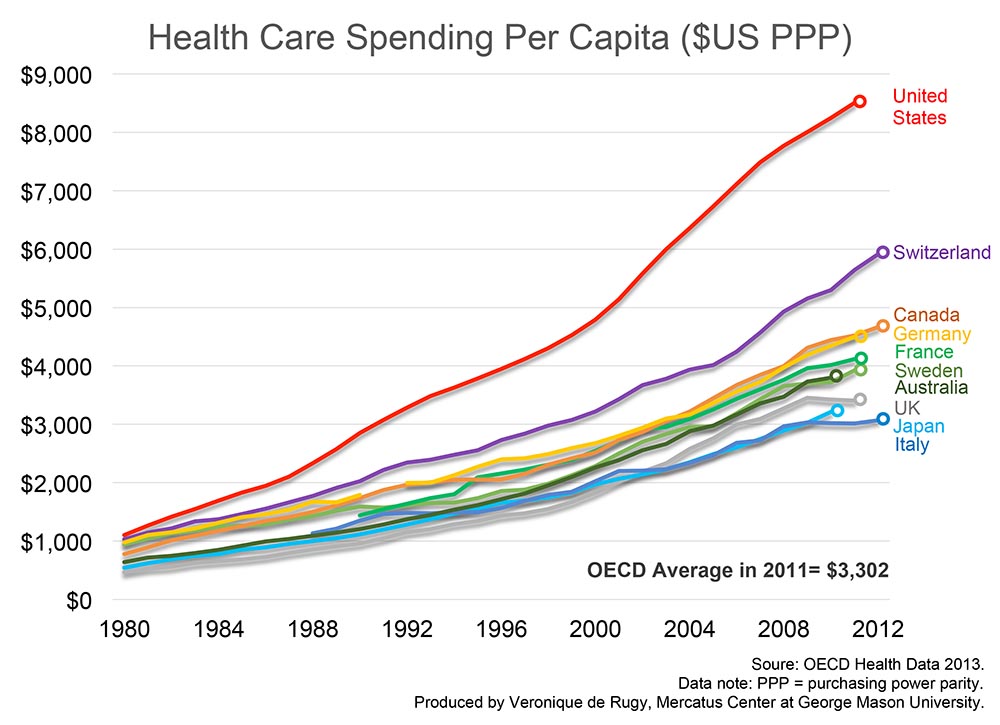
What’s the point in arguing over details? The reality is the American health care system costs an average of about $8000 per person per year and the Canadian health care system costs an average of about $6000 per person per year. And their system is providing better health care.
So why argue about where that extra two thousand dollars is going? Let’s just adopt the Canadian system and start spending less money for more health care.
Did you hear that, America? Democrats want to kill 600,000 good jobs so you can have the “luxury” of socialist medicine. Inform your church and rotary club!
Here’s another conservative argument in favor of a public health care system: it encourages entrepreneurship.
Under our current private system, a large number of people get their insurance through their employer. This ties people to their jobs. A person who might otherwise have the talent and resources to start his or her own business might hesitate in the face of the huge risk of health care. Insuring yourself is a crushing expense. Being uninsured (or having your family be uninsured) is an unacceptable risk. So people are forced to play it safe and stay in their current jobs. And our economy loses all the benefits that we would have gained from those new businesses.
Once again, I don’t know about all UHC systems, but at least here, I most certainly can pick whichever specialist I want.
Can you point out to an UHC system where people can’t pick their physician? You seem to be bent on arguing that it’s legimate concern, which doesn’t make sense if you don’t know about any such system (and hardly make sense even if you do, since why would you expect the USA to pick such an unusual system?).
Plus these two hospitals can charge very different rates for the same procedures. Letting market forces take over - as has already begun with the publication of a selected set of rates - will drive prices down in the more expensive suppliers, and make them more efficient.
You need to carefully read post #37 by Grim Render, which is an excellent description of where all the extra costs are, a point I wanted to make anyway – it’s a post well worth reading and understanding.
The most striking difference between the medical systems in the US vs Canada is the absolutely extraordinary amount of paperwork and bureaucracy associated with private insurance and the staggering amount of manpower devoted to it – or conversely, the almost complete absence of it in single payer. The impacts are enormous and cascade down throughout the whole system – a major reason US medical providers charge what they do is to cover the costs of maintaining a collections staff and covering the costs of being stiffed by insurance companies. When a public insurance system can guarantee full payment without any hassle, they have significant leverage to negotiate much lower base rates, which not only establishes a lower cost structure but is also a safeguard against gouging. The end result is the cost structure you see in every advanced country in the world, an average of about half the per-capita cost in the US.
On the subject of choice in doctors which was mentioned several times, some countries with mixed public-private insurance systems have public sector and private sector providers, and how this plays out depends on the country. All Canadian provinces conform to the Canada Health Act requirement for providers to take single-payer coverage for medically necessary procedures without extra billing. There was once an opt-out loophole and it may still exist but in practice there is no private-only sector providing medically necessary procedures. So essentially you have complete freedom of choice among doctors, who are generally in private practice, and any hospital you like. It’s exactly the same choice you’d have if you were paying out of your own pocket. It’s ironically the private insurance system that imposes “in-network” requirements, which can be onerous especially if their “network” is particularly limited.
That does work to a degree for care that is not medically neccessary, such as lasik and vanity surgery. However, basic Health Care Economics says it does not work for most health care and all real-world experience backs that up. Ask out UK posters what happened when they moved to competition-based dental for example.
The fundamentals of Health Care Economics wes formulated by Kenneth Arrow as part of the work on uncertainties that got him the Nobel prize in Economics. The paper is still available online.
That’s going to be part of reducing payments to health care providers.
Combined with tort reform, rationing is the only realistic option to reduce health care inflation.
Actually, it does, in part, because Obamacare was going to reduce costs borne by the insured and incurred by the uninsured. As well as allow Medicare cuts. Or rather, increases in Medicare spending that are not as large as they might otherwise be.
Regards,
Shodan
If it were that easy to make doctors and hospitals take a 25% cut, I suspect that Congress and private insurers would have done so already. No system anywhere has been successful in actually cutting healthcare costs; the best anyone can manage is restraining growth, and we now do that as well as anyone. We just have higher costs baked into the system based on past cost growth, and switching to single payer isn’t going to change those in a significant way.
It’s an interesting theory, but do we really think European economies are more entrepreneurial than in the US in practice?
On what basis do you claim that “we now do that as well as anyone”? ISTM that despite the ACA, nothing structurally has changed, and particularly nothing in terms of oversight of provider rates and the reasons they need to be so high, as previously discussed. This chart pretty much says it all. The only curve that is close to the US rate of increase is Switzerland, and IMO Switzerland has some of the same issues as the US due to the prevalent role of private insurance. I see no reason to believe that the same factors that “baked high costs into the system” aren’t still baking away, as hot as ever.
{kind=link}
No, but for socioeconomic and cultural reasons unrelated to health insurance. Everything else being equal, health insurance considerations just increase the risks of leaving a job and plunging into self-employment, especially to a person with family dependents.
who the heck said anything about making doctors taking a 25% pay cut?
The underlying problem with the idea that UHC would fix the national is that healthcare does not in and of itself compound the debt. Insurance is a very big industry, employing millions of people, many of whom pay taxes on the salaries they earn from trying to fuck you over by denying your claim. Institute UHC and most of those jobs will evaporate, leaving a bunch of Americans looking for work and erasing a couple million in revenue. The money we all would save would be a good thing, but it would not go toward addressing federal deficits or debt.
Same old same old. When the facts disagree with ideology, American exceptionalism will be claimed as the reason why universal health care could not work in the USA.
It this simple, folks: you are paying to support an extremely inefficient but highly profitable private insurance industry.
I’d suggest that Canada has a significantly better health care system than the USA, and that Canada still can do a lot to improve it’s health care system even more.
Wow, this was a very lucid summary of where so much of the costs are located. Which begs the question, How do you convince conservatives that we have a problem in the first place?
My pet theory is that most of them don’t want to do much reading and analysis, hearing about government interventions as part of a solution and automatically discarding that as making things worse is their lazy way out. They don’t have to actually think the problem through, but we need them. We can’t change this on our own. The other lingering issue is path dependency. Given the cobbled mess we currently have, what would be the best system to move towards to make the transition easier and less destructive, even if the local minimum is not quite as low as some other ideals.
You already have rationing in the US. It’s done by the insurance companies, who decide what doctors you can see and what procedures will be covered, as well as the amount that the patient has to pay up front, by way of premiums and co-pays.
Doesn’t seem to have kept costs down.
Also, why the linkage to tort reform? Adaher made a similar one line comment in the Ben Carson thread and I didn’t get it there, either.
We’ve done this before on the SD and I think that poster was pretty accurate.
This shows just how ugly the situation is and how you get to spend 50% more for lower life expectancy:
https://www.washingtonpost.com/news/wonk/wp/2012/09/07/we-spend-750-billion-on-unnecessary-health-care-two-charts-explain-why/
With regard UHC, the great cost-cutting driver is the public really, really like getting a lot for their money. They’ll vote for that.
It’s just a question of how serious one wants to be about cutting costs. As noted upthread, if one looks at the numbers, the administrative costs of private insurance are a drop in the bucket of health care spending. It’s of purely symbolic political importance, like tort reform on the right.
The problem isn’t insurance; it’s that our actual health care system has much higher costs baked into it for historical reasons. We can’t cut costs unless we cut what we spend on doctors and hospitals, and no system anywhere in the world has been successful at doing that.
Hmmm, I must have missed that - I saw the opposite noted. Could you point it out to me?