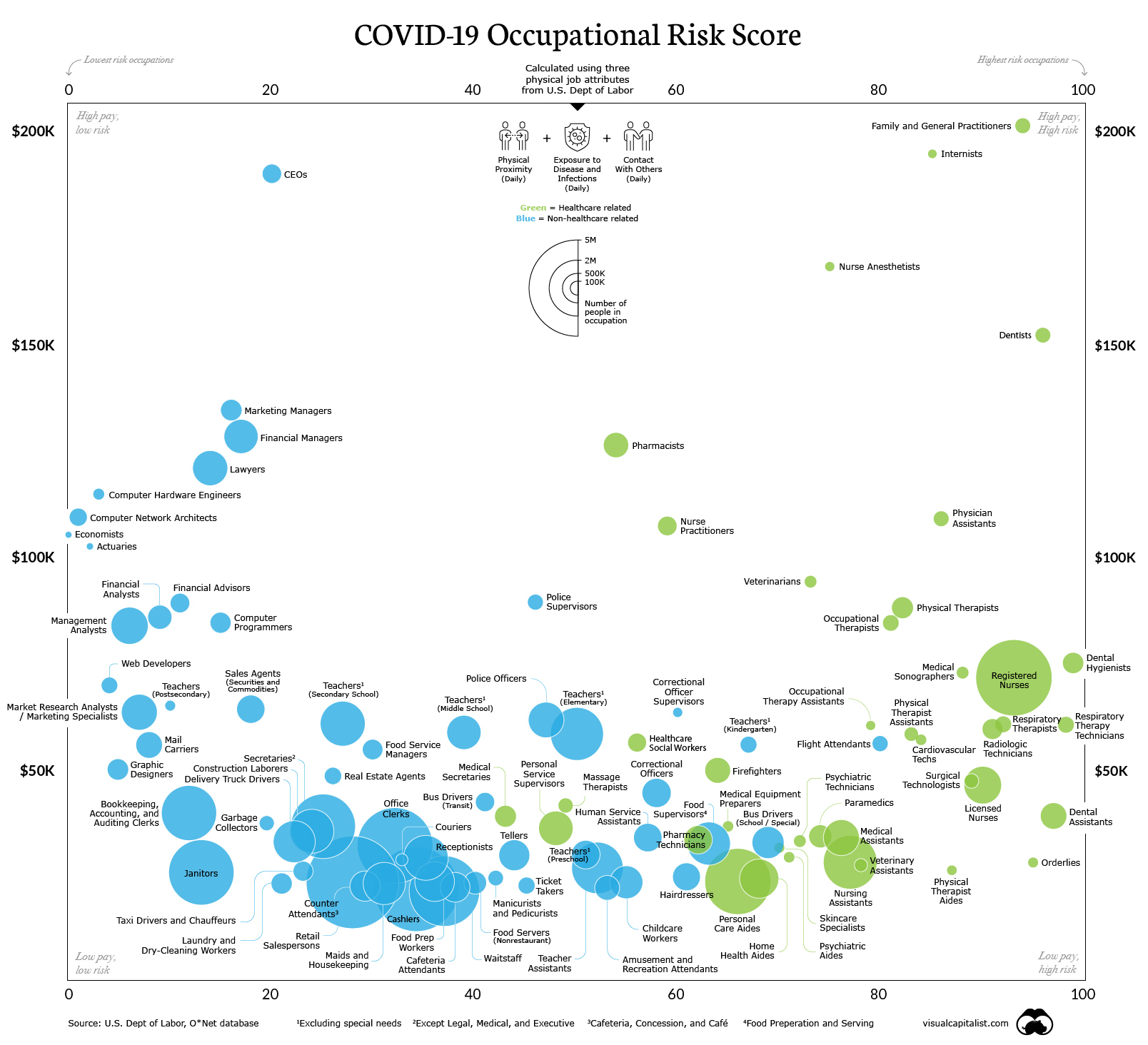
Couldn’t find an existing thread that this would sit in (it’s not breaking news) but this graph is very interesting. Flight attendants are the most at risk non-medical group although in France I’ve heard that taxi drivers were at the top and they are considering using occupation as a way of deciding vaccine priority. Dental hygienists have the most at risk occupation.
Despite having a whole category for “medical-related”, it looks like the only physicians on the chart are general practitioners. What about all the other specialties?
And is this based on models or empirical data? I’d think that there’d be plenty of empirical data by now, but it looks like it’s calculated from a model?
Also, what exactly does “risk score” mean? It’s on a scale of 0 to 100-- Is that percent chance that you’ll get the disease? Over what span of time?
This, I think, backs up my decision to put off non-urgent dental visits. I went in once during the summer when I cracked a tooth, and they had me sign a waiver detailing essentially how great a risk there was. It was sobering. Saliva is aerosolized from the procedures, and as a patient, you are sitting there with your mouth open – no mask is possible during the procedure.
Hygenists’ procedures probably aerosolize the most saliva. Exposure risk would be high, especially if PPE was scarce or imperfectly worn.
Our flight attendants (all 20,000+ of them) have been getting sick at the same rate as the general populace. This has been true since COVID began.
An awful lot of them are from COVID-denying parts of the country and it’s reasonable to assume they behave unsafely off duty at about the same rate as the general populace wherever they live.
What do all of them have in common: whether pro- or anti-mask at home, while at work they are very serious about this stuff. Management is on everyone’s ass & hard.
What I conclude is the precautions work when everybody uses them. Despite being stuck in the airplane, hanging out in airports, restaurants, and hotels half the month, they aren’t getting sick more often than the general populace.
Yes. It is, unfortunately, completely theoretical, and has been obviously wrong: it postulated that people who come into close contact with lots of different people for short periods would be more at risk, but the actual high risk has been associated with people who came into close contact with the same people for long periods.
It missed the distribution characteristics of the epidemic, which as I squint at it, makes it seem likely that it will be a better predictor for the next 6 months than it was for the previous 6 months.
Hard to find any studies. One of the only ones I can find is this UK study from the summer but it looked at death rates not infections, and it bunches occupation into occupation type (such as “Elementary Occupations” like cleaners etc). i.e. this is a study that tells us how likely you are to die if you contract covid by occupation which must be caused by several factors.
There’s this also from the UK’s Office of National Statistics, but I think this is also based on an estimate so is very similar to the one I posted (it might even be derived from the same data). The charts here are interactive:
A couple of months after that report the ONS released another report looking at actual death rate numbers but only had a couple of paragraphs about occupation.
[The] ONS reported that men working as security guards, taxi drivers and chauffeurs, bus and
coach drivers, chefs, sales and retail assistants, lower skilled workers in construction
and processing plants, and men and women working in social care had significantly high
rates of death from COVID-19. Our analysis expands on this and shows that nursing
auxiliaries and assistants have seen an increase in all cause deaths since 2014 to 2018.
For many occupations, however, the number of deaths is too small to draw meaningful
conclusions and further analysis will be required.
Not sure if all my search results coming from the UK are to do with my location or because nobody else is publishing stuff.