I went to my GP for my first post-50 physical. He asked me a bunch of questions, tapped a few things, listened to some others, EKG, etc.
All was good, and then off to the blood and urine tests. He called me this week with the results. Everything was good, except that I’m very low on Vitamin D and my cholesterol is 260. He told me to buy some OTC Vitamin D pills and to “get your cholesterol down”. I’ve had high cholesterol for a while, but more like 220. However, I’ve also always had a good ratio, which I’ve read is more important. But I figured it doesn’t hurt to try to get it down, so I asked him how. He said to cut down on dairy. I’m already lactose sensitive, so don’t drink milk. I responded that my Vitamin D is low, and the only real dairy I consume is the cheese on my pizza and yogurt. He said cut down on pizza and switch to “low cholesterol yogurt”. Does that sound right?
I’m always skeptical of old doctors, as I don’t believe they get enough continuing education. I’ve gone to specialists armed with more current knowledge of their fields than them. So would love to hear opinions on both the Vitamin D and cholesterol issues. On the latter, he never mentioned anything about Lipitor or anything. A few years ago, he threatened me that he’d have to prescribe it if I didn’t get it down below 220. This time it was 260, and he never mentioned it.
General practitioners have essentially no training in nutrition beyond pathological deficiencies, and as you note continuing education is often lacking for GPs, especially with regard to nutrition. Although it was once assumed that the major source of cholesterol is from cholesterol-containing foods, in fact dietary sources of cholesterol have relatively little impact upon production of cholesterol in the blood. What is more important is preventing hormonal disruption that stimulates cholesterol production, and specifically by eating foods high in soluble fiber and monounsaturated fatty acids, and low in processed carbohydrates.
The use of statins like Lipitor or supplements such as cholestyramine as an intervention to control cholesterol levels should be reserved for situations where dietary modifications are not achieving the desired reductions because of the many adverse side effects these can have.
Are you overweight? I found that losing weight had the strongest correlation to reducing my cholesterol, diet had little effect. As I understand it, some people just have a genetic disposition to high cholesterol and statins are really the only way to reduce it. Fortunately for me, I was able to reduce mine by losing weight.
I don’t think I’ve ever been described as overweight, but could probably stand to lose 5 pounds. I’m 5’ 9” and 170 lbs., but also relatively muscular for my age, both naturally and since I lift weights. I think 165 lbs. would be my ideal weight.
When I was in my 30s my total cholesterol was 239 and my PCP happened to be a cardiologist. He put me on a low-fat diet and exercise, and then tried some OTC meds like Niacin, and nothing worked. I could get it down 10 points, but it was hard work and never got close to being under 200.
He then decided to put me on a statin, and within a month my TC was down to 169 with no side effects and I could eat anything I wanted. That was 37 years ago and I’ve since learned that my issue is genetic and diet and exercise can’t 't fix it. Unless you are against taking a daily medication I don’t know why your doctor wouldn’t suggest it. It’s safe and it works.
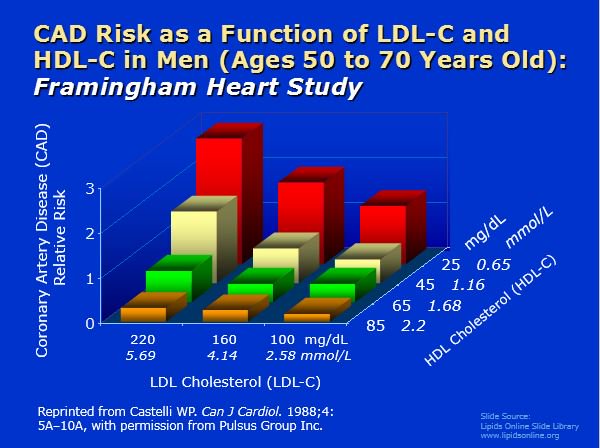
This old Framingham data nicely demonstrates that even for a man with a high LDL of 220, the risk of coronary heart disease (CHD) is less than average so long as his HDL is greater than 65.
Notice also that for a given level of HDL, as LDL goes from 100 to 220, the relative risk of coronary disease increases by two- to three-fold. On the other hand, for a given level of LDL, as HDL goes from 85 to 25, CHD risk increases as much as tenfold. IOW, this observational data suggests that HDL is more important than LDL with respect to coronary risk.
Another point to make explicit is that this data would seem to suggest that, sure, your CHD risk increases as your LDL levels increase. But if your HDL is high (> 65), lowering your LDL from 220 to 100 has only a minor effect on your risk (and even at that, takes a person with low risk to very low risk - sorta the law of diminishing returns).
I guess all of this is just another way of pointing out that the LDL to HDL ratio (or total cholesterol to HDL ratio) would seem to be more important than either alone.
The bounds on this and similar charts explain why my PCP is stumped by my lipid panel. HDL on its own flags danger, but LDL is <50. “Eat more [describes my current diet],” she says.
My numbers aren’t too different from yours. My physical last August showed that my cholesterol was high but also with a good ratio, 276 total, LDL 175, HDL 73. My GP, who I like, said to watch my diet (I’d been eating cheese, beef, liverwurst, cold cuts) and add more fruit and veggies, exercise a bit more, take psyllium and Cholestoff.
I wasn’t overweight, 5’4" and 135 lbs, BMI 23. High cholesterol runs in my family; my sister is thinner than I am but her doctor has her on statins. She has an additional risk factor, though, being a smoker.
So I went back last week, having followed his advice for a year and hoping that the numbers would be better. My weight hasn’t changed but I’m down to 240 total, LDL 154 and HDL 70.
My doctor was pleased and said to keep working at it. He suggested another OTC option, especially if I’m tempted to eat some of my old favorites again: Red Yeast Rice capsules. I haven’t started them yet but the reviews look good.
For decades, my overall cholesterol has been slightly high, but my good cholesterol ridiculously high.
I’m pretty much content that my weight/health is decent, I get sufficient exercise, and my diet is pretty good. Of course, I could exercise more, eat less crap, and more good stuff - but I know that independent of any single statistic. I’m not interested in really modifying things in pursuit of one specific numerical value or another. Having some specific cholesterol value isn’t gonna make me live forever. Something or another is gone kill me.
My doctor said that he didn’t think my numbers were high enough to warrant taking statins especially with my ratio, my lack of other risk factors, and with the possible side effects of statins. Here’s some lines from an article with a number:
“The most important thing your doctor will keep in mind when thinking about statin treatment is your long-term risk of a heart attack or stroke. If your risk is very low, you probably won’t need a statin, unless your LDL is above 190 mg/dL (4.92 mmol/L).”