First off, this is a question to aid my morbid curiosity, not a request for medical advice (firstly, my b-i-l is a few thousand miles away, secondly I have no reason to doubt the quality of the care he’s getting, thirdly I do respect that a message board is not the place to ask for medical or legal advice ).
My brother-in-law took a major tumble off his bicycle a few days ago and broke his right elbow and right humerus (and a couple of fingers on his left hand, but that’s a minor concern). I guess the damage was reasonably significant - he had surgery yesterday. My sister (his wife) said that they had to break his humerus further up as part of the repair. This was apparently mentioned more than once, making me think that it probably wasn’t a misunderstanding.
So, my question. Assuming there was no misunderstanding, why would they need to make a new break surgically in order to repair his existing breaks?
More minor question - given a badly broken humerus and elbow, how long is it likely to be before it’s as better as it’s ever going to be?
I have a friend who suffered the same injury, and my response is based on that. I am not a doctor, etc.
In humerus fractures, one of the complications that can occur is the radial nerve becoming entraped… in my friends case, the bone was reset in a way that pinched or otherwise impeded it. If that problem is left uncorrected, you won’t have full motion in your wrist and fingers.
Predicting recovery time would require knowing many other factors, but for my friend it was 3-4 months, and at some point in that process he had started physical therapy.
Most humerus fractures do not require surgery, and the fact your bil’s did implies significant injury. This could include radial nerve damage, as stated. Surgery is usually indicated for open fractures (the skin is open to the bone), foreign bodies in the arm (e.g. broken glass from a car window), significant linear or angular displacement (so that the bones are not abutting at the break and won’t heal well), when there is damage to the arm’s blood supply (artery or vein), or damage to the bone (avascular necrosis) secondary to poor blood supply. The arm might also be rebroken if the original diagnosis was delayed and healing had begun while the bones were in a poor position.
The term “rebreak” has always struck me as pretty melodramatic. Most fractures in the operating room have not healed significantly, and do not take much force to rebreak.
As Dr_Paprika says, “rebreak” seems to be a misnomer of sorts.
I’ve been in the OR during many, many fracture reductions, and I’ve yet to see the surgeons (intentionally) re-break a bone before applying the fixation.
Now, I have seen a bone broken in the OR, but that was when the ortho doc was placing the pin down the shaft of the humerus and it fractured. That was certainly not the desired effect, though.
There have been some cases where a previous injury, now healed, has been causing some kind of pain or impairment and the docs have gone in to re-allign things, but I don’t think of those as “rebreaking.” More like remodeling. They don’t just manually snap it, reallign it, and pin/plate it. They’d use a saw to cut it before they’d just take a hammer and chisel to break it. Once things were in better allignment, then they’d fix it in position.
Thanks guys! That helped my understanding a bit. I don’t think he had an open fracture (I’m sure my sister would have specifically mentioned something that gruesome), but apparently she could hear “crunchy” noises in his upper arm if he even moved his hand. The incident was Tuesday, the surgery was Friday.
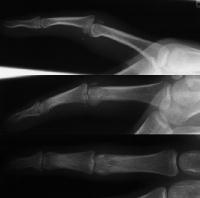
Based on the “crunchy” noises, I think your friend’s fracture may have been comminuted, or broken into several pieces, two long ones and a bunch of tiny ones. Some of the tiny ones may have become dislocated (X-ray, not squucky). The caption for that picture says “Xrays show a comminuted dorsal fracture dislocation of the proximal interphalangeal joint with dorsal subluxation”, meaning the pieces are not only broken and small, but out of place.
Rather than “rebreaking” the bone, the docs may have had to rearrange the fractured pieces and even excise some of the smaller ones so they could get wires through them, something like this x-ray. (Notice there’s not only wires and other hardware in the arm, but a lovely staple line at the skin closure site. Loooonnnng skin closure site.)
I admit this doesn’t explain why several people associated with your friend used the word “re-breaking”.
Thanks. My sister is trying to get a copy of the X-Rays. If she can, I’ll be able to look at them later this month (for other reasons I’m probably heading their way for a visit).
My experience suggests patients just like to use the term rebreak. Plenty of people enjoy being melodramatic about their injuries (they really do, I’m not being incompassionate) , and this term implies a “seriousness” not always justified. Our emergency pay phone is located near the desk and while I don’t make a habit out of eavesdropping on conversations, it is interesting to hear what patients tell their families, bosses and friends after I’ve seen them.
and about their health in general (well, at least, many people).
I still think it’s “cute” how, when I’m taking a patient’s history, virtually everybody feels compelled to use the term “rushed”, e.g “Three years ago, when had I chest pain, they rushed me to the hospital” or “There was that time in the 1980’s when I had to be rushed to the hospital when they thought I might have be having a stroke”.
In my family, before I went to medical school, there was a definite air of competition for the rarest, most unheard of disease. “Well, I’ve got an X and my doctor said it had never been heard of before!!!” to be topped by “Three doctors never heard of mine before!” and “Mine stumped five medical students, six residents, and an attending at Harvard!”
It wasn’t until I got into medical school that I discovered this meant rare bad luck, i.e. the diseases the doctor can best you treat you for are the ones about which medical science knows a lot. The commoner your disease, the likelier that there are known risk factors, course, progression, and cure.
Took a while to turn my head around the appropriate 180 degrees…
 ).
).
{kind=link}
{kind=link}
{kind=link}