I think hospitals still have cheap analog phones (like this one) for patient to use to make phone calls. But both of my parents have been in hospitals or long-term rehab in recent years and they brought their own smartphones with them, with a long USB cable plugged into the wall behind the bed. So my idea for an improvement would be for the beds to have a built-in USB charger, so the patient’s phone can be nearby and charged.
Private and semi-private rooms have become commonplace in hospitals in only relatively recent times. Privacy is not something hospitals were historically known for. The flowers are a nice touch though.

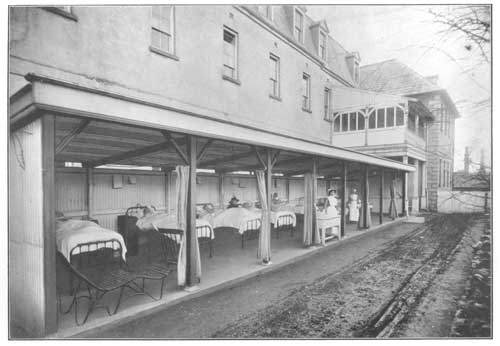
True, old-time hospitals had some innovations that modern facilities have overlooked, like open-air wards for TB patients.
‘At first it was thought that the patients would not like it, especially in the winter time, but this was found not to be the case, and during both winter and summer there is keen competition for a bed in the open-air ward.’
Kirkpatrick (1924), History of Dr Steevens’ Hospital, p. 321.
That’s actually an interesting point. Apparently I was on the trailing end of COVID when I was admitted; about a week prior to going to the ER, I had started a cough, which was pretty dramatic for about two days, and then turned into an intermittent, every hour or so cough. Fever for a day, and that was about it. I wondered if it had been COVID, but it never seemed serious enough to actually test and isolate while on vacation- I’ve had worse coughs and congestion from breathing too much campfire smoke in the past. Vaccines and boosters for the win I suppose.
So they stuck me in the negative pressure rooms up in the COVID floor. I kept having to remind the nurses and doctors that no, I wasn’t in the hospital for COVID, but for the arm infection. They put me through the whole battery of oxygen saturation tests and cautions, etc… and were kind of surprised when my saturation was higher walking and talking than just quietly sitting.
COVID has sort of screwed up their perceptions in that ward- they were having a hard time getting around the idea that COVID wasn’t my problem, no matter how many times I told them that I only knew I had it because they tested me for it and that I could breathe fine, etc…
Ha ha. I didn’t find the actual device uncomfortable, just sufficiently distracting that it was hard to get to sleep. Someday I may reconsider.
A question about the old photos of hospital wards: when did mechanisms to raise or lower beds come into usage? Way back in the dark ages, I was a Candy Striper at a hospital in which beds in one wing still had cranks to raise or lower the foot/head. I’ve read books written in the 1950s that mentioned those cranks, so I know they go back that far. The beds in the photos upthread don’t seem to have any mechanism for doing so. And wow, those mattresses are thin!
I would suspect the earliest models would have adjustments like sunbathing recliners, where you have someone physically move it up a notch. Or someone would just prop you up with pillows if necessary, which I believe the photo shows.
Here’s the thing though, you are not the only patient there. The schedule has to accommodate everyone. I am retired now but when I was working as an RN (30 years on the night shift) we would do everything we could to try to give the patients as much uninterrupted sleep as possible. But the priority of course is averting crises, and that requires pretty close monitoring sometimes.
I didn’t read the entire thread, so I apologize if this has been mentioned, but I know the reason for the 5am blood draws. It is so the physicians will have the lab results available to them when they make rounds each morning.
Most everything else that has been questioned is very likely due to dollars.
mmm
My dad grew up sleeping in a bed on his parents’ front porch, almost exactly like the beds in that photograph. Throughout his life, he would open up every window in the house, weather permitting. (And his notion of “weather permitting” was a lot more expansive than Mom’s.) If he had been in a hospital with an open-air ward, he would have begged for it.
I had some stents put in five or six years ago and was similarly impressed by the experience. Since I was only under a local anesthetic I was able to hear the doctors and technicians as they discussed what was being done, what they were seeing, and deciding that there was sufficient blockage in two places to warrant placing stents there.
My only complaint was that I had been given the impression that I would be able to see the progress of what was being done, but none of the screens were positioned to allow that.
My (Canadian) employer offered supplementary health insurance to cover the stuff the government didn’t pay for (mostly glasses and dental), which had 3 levels of monthly premium, differing only in whether they covered private, semi-private, or general ward hospital accommodation. I changed mine from semi-private to basic level after my first hospital stay, when a nurse informed me that all the local hospitals were being gradually renovated to eliminate the four-person wards, and all the single rooms were reserved for infectious patients. Two-person rooms were the default regardless of what you or your insurance were willing to pay.
There’s absolutely some institutionalized cluelessness built in.
I have literally had a 100% error rate on my medications - both times (aside from childbirth) where I spent a night, my maintenance meds were botched. Other orders were messed up (e.g. the time I was supposed to have continuous pulse ox monitoring, and the doctor DID order it, the nurse refused to do it saying it was not standard). Oh, and the doctor ordered an anti-nausea medication that was explicitly proscribed in my case - luckily, I did not need anything for nausea, or there would have been hell to pay. The first hospitalization, I was sharing a room with an incontinent elderly woman who had a potty chair in her room - I had to go down the hall to pee. Nor did I receive my pain meds on time.
I genuinely believe a hospital is no place to be if you’re not feeling well. Yeah, I know, sometimes you truly do need the skilled care - but it’ll be a cold day in hell before I spend another night in a hospital, and I WILL have a family member with me the whole time, to protect me against the truly stupid errors made by staff.
Then there was the time after my second child was born. I spent some time in the ICU afterward because I’d been attempting to die, before she was born (pre-eclampsia). Doc forgot to write the order saying I could be discharged to a regular room after x hours. We made the staff wake her up at 3 AM to correct that oversight. Then I got moved to a regular room… and the BED malfunctioned, requiring a swap at midnight.
I loathe hospitals.
Perchance were you a guest of a military hospital?
I requested a pain pill, and the ward tech who answered the call said I’d have to walk down to the nurse’s station to get it, because there was only one nurse on duty that night.
~VOW
That reminds me of the time when I was in labor with my oldest. I had tried to get an epidural but the anesthesiologist could not get the needle in my back. So I was just trying to white knuckle my way through induced labor. About 3 hours before the baby was born, a random maintenance guy came by and asked if he could change the toilet paper dispenser. I was obviously in no mood to be distracted from breathing but I said OK. Then the guy, apparently freaked out by what was happening to me, hesitated in the room just watching for what felt like an eternity. I yelled at him to hurry up and he did.
Not long after that, the student doc came by to check on how I was doing and I told him I needed to push. He started walking calmly out of the room to get the big doc and I yelled at him to run, not walk, as I was about to push a baby out. Baby came so fast my doctor made a surprised noise.
In the final year of my mother’s life, i did this. I sat in the hospital room with her most of every day during her several visits there.
I was not - but I did actually wind up walking down to the nurse’s desk to ask for it, after my 4th or 5th request had been ignored!
Sadly, this is genuinely necessary in many places.
The last time I spent the night in the hospital, they put me in a room with someone who was suffering from some brain issue. I think he had been in a car accident and he was completely out of his mind. He wasn’t strong enough to stand and walk on his own, but he was convinced he had to leave to go to work. Every time he tried to get out of bed, the whole room rang with alarms and warning announcements. It was pure torture for me. I couldn’t imagine why there wasn’t some accommodation for hte situation that would allow me to sleep.
Lucky you. Really.
I remember finally asking for pain relief about 5:30 AM. This was an induced labor, attended by the Nazi Doctor From Hell, who did NOT use steps to prepare the cervix (my water had broken, so induction was not optional). They find something or other, and I asked “Does it have sulfite preservatives?”. It did. Doc tried arguing “What will it DO to you?”. I snarled “I don’t know - and I don’t think NOW is the time to find out”.
They found an alternative - but then said maybe I’d love an epidural.
It took the anesthesiologist 90 minutes to arrive.
He refused to stop for 30 seconds when I had a contraction. “If I did that, I’d NEVER get done”. Then he botched it so badly I screamed in agony and jumped. To the best of my knoweldge, that was the only time I screamed during the whole process/ The nurse, who was NDFH’s soulmate, snarled at me for moving.
And they refused to believe me when I said it was not touching the pain. I can bloody well tell the difference between “pressure” and “pain”. fuckyouverymuch. This was quite entertaining when they started talking about an emergency c-section.
They actually redid the epidural when they did a last ditch effort to get the baby out with forceps. So at least the 3rd degree tear didn’t hurt, when they were putting me back together.
I detest hospitals, you might have noticed. I’ve told my husband that THAT hospital in particular, should I ever wind up there in an emergency, he is required to have me moved - to pretty much anywhere else on the planet - as soon as I’m anywhere near stable enough to move. This is the hospital that fraudulently billed for an extra day stay, too.
My mother in law who I loved dearly was dying of cancer. She was frist admitted to the hospitals cancer wing (before things were obviously not going to get better) and received excellent compassionate care in a single room. Fast forward a few months: she was admitted to a general ward in the same hospital. She begged me to stay the night. I think she knew things were winding to the end and was afraid. This section of the same hospital was a joke. It was a semi private room. The woman in the other bed appeared to be unconscious. This poor woman’s IV alarm would go off about ever 15 min. to 30 min. The nurses station was less than 15 feet down the hall. The alarm was extremely loud and no would come and check it and or turn it off until I buzzed them several times. They were very annoyed to be pulled away from the gossiping and laughing they were all enjoying at the nurses station. I was so glad I stayed, she got little sleep that night, but she (and her room mate) would have been completely ignored if I hadn’t been there. And I wondered why the staff were very unenthusiastic about me staying.
I’ve had overnight hospitalizations in Singapore and South Africa, of 1-4 nights each time. Overall, I’d give all experiences high marks. However, in South Africa (in 1998) I was in a “private” hospital. I gather that the level of care there was far higher than what a citizen who couldn’t afford such care would get. (Perhaps a knowledgeable person like @MrDibble can weigh in. Would a Soweto resident thrown on the mercy of whatever hospital they could access receive the same care? In 1998, or now? I could speculate, but my understanding is limited, so I won’t.)
I will say that the care I received in SA on the birth of my child was less racist than I would have expected. My OB-GYN (who was Afrikaans) had plenty of Black patients in his waiting room; in fact I recall at least one time when I was the only White person there. However, I had chosen him because I was told he was progressive; maybe he wasn’t representative. I’ll never know as he saw me through my pregnancy and delivery, and then I left the region.
(A side note, not an answer to this thread: my roommate in the hospital was Swahili. She cried constantly. Her avuncular White doctor asked her how she was doing. She snarled, “how do you think? This is my third girl! My husband wanted a son.” Having just given birth to my first and only child, a boy, there was nothing I could say.)
Singapore had amazing care, but again, that was almost certainly because I was privileged. Singapore citizens and medical tourists undoubtably receive excellent care at prices that are remarkably low compared to the bloated American health care system. Do struggling immigrants who clean filthy bathrooms and dispose of garbage for pitiful wages receive the same level of care? I doubt it.
That’s only two data points and I wouldn’t generalize to the whole world from that. How do Scandinavian countries do with economically sound citizens vs immigrants and/or the poor?