Health care interests spend more in lobbying and political contributions than military and energy combined. (Source - the Atlantic from a couple of years back - sorry, no specific cite/link available).
I agree with Shodan, that some degree of rationing is needed. I do not understand how it is sustainable to have everyone eligible for essentially unlimited care, with providers encouraged to provide as much care as is covered.
I am talking about rationing based on cost-benefit analysis. As in “no, we are going to let your 1500 gram newborn die” or “the waiting list for a hip replacement is six months - you will have to manage somehow until then” or “that drug may work 10% better, but you can’t have it because it costs too much” or “we don’t cover mammograms for women under 50” or “statin drugs don’t affect life expectancy so we don’t cover them”.
We need to ration more by cost and less by medical consensus. Because we need to accept that a certain number of people are going to die that wouldn’t die if we continue to pay for everything. Medical consensus is always going to come down on the side of doing more. We need to do less.
Does that mean more people are going to suffer and die? Yes, it does. But we want to save money. So we have to accept that.
You understand that a certain amount of people die who would otherwise actually be very cheap to save simply because they don’t have effective access to medical care, right? It’s not like going to single payer would suddenly result in a whole lot of people being killed - on the contrary, it’s likely to save a lot of lives simply by giving people access to care. The difference between someone having no care to having pretty good care is a bigger difference than denying someone a drug that’s 10% more effective but costs 5 times as much.
Also, everything you said just seems sane to me and we should realize that whether we go to single payer or not. It’s ridiculous how we’ll spend millions of dollars on broken down elderly people in their last year of life while lots of young healthy people go without very cost effective care.
But these things aren’t really related. If we had a net savings by going to single payer because of collective bargaining power and administrative efficiencies, that’s more health care available to everyone.
More billing staff than than doctors :eek:. And this was presented as a model of billing efficiency! I’m not quite sure how to express how gob-smackingly inefficient that sounds.
Comparing the cost of sending it out to a 3rd party service was harder with just a quick google. But this document (warning, PDF, info on page 41), which seems aimed at new Canadian doctors suggests that 1.5% - 4% of gross revenue is the expected range. I found an American services willing to put 7.9% - 10.9% on their page :eek:! Others, who were actually willing to post prices publically, had ones in the rage of 4% - 8%. No doubt the insurance companies receiving these claims are also spending a lot more to process them than the Ontario Health Insurance Plan is too.
It certainly looks like there’s costs that could be cut on a move to single payer. (with a lot of laid-off medical billing staff at a minimum)
Yes, those numbers sound about right for the US market.
I don’t think it’s as big a deal in total care costs as issues like US use of MRI machines being two to four times as high as the equivalent use in Europe, but billing is one of those elephants in the room that neither political party wants to talk about.
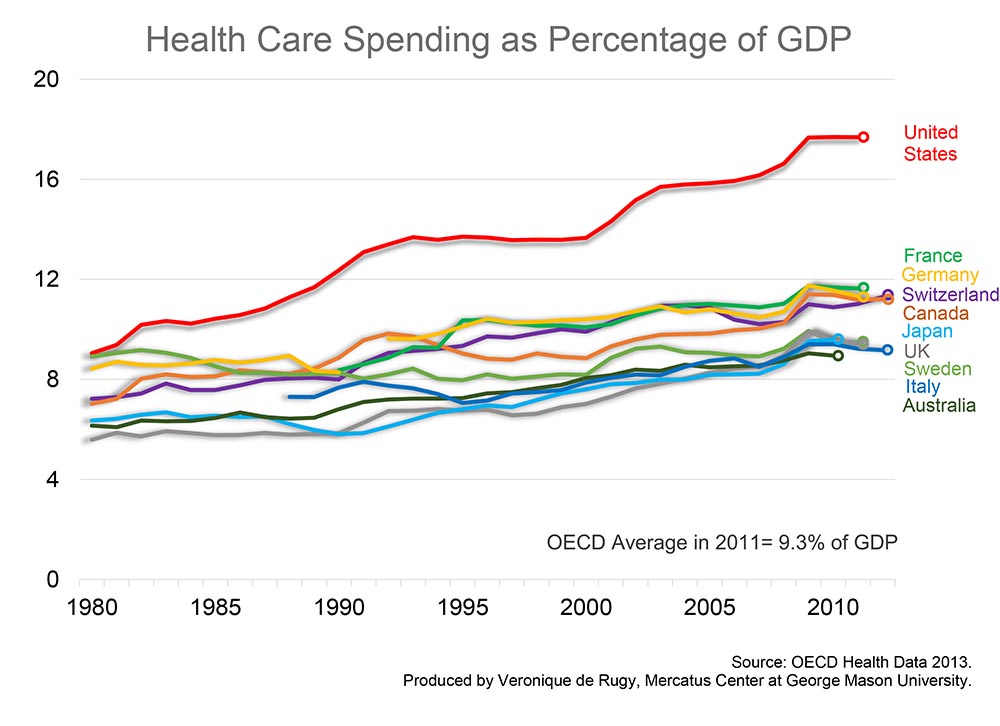
That chart is health spending as a % of GDP for various OECD nations. Back in 1980 the US spent 9%, now it spends 18%. That is a 9% increase. Most other OECD nations saw their % devoted to health care go up by 1-4%. France went from about 9% to 12%. Germany went from a little more than 8% to a little less than 12%. Israel, FWIW, has had a consistent 8% for decades. Had our health inflation spending been in line with other OECD nations we’d spend about 12-13% now instead of 18%.
So the US is an outlier, our health care costs have skyrocketed since 1980 compared to other nations. There were a lot of tech advances in the last 36 years, so that cannot be the main/sole reason prices have gone up, because they have gone up far far less in other wealthy nations. Some nations that adopted tech advances and saw their populations age saw health costs go up 3%, some like Israel saw a 0% increase. None saw the 9% increase the US did.
Rationing is really not a bad idea considering that 30-50% of our health spending doesn’t actually make people healthier. However separating that from the other 50-70%, and cutting it isn’t easy.
It can work in the US. The people who say it can’t work usually just say that because they have a financial or ideological opposition to having the public sector be involved in health care, and pretending the US is too big for single payer to work is the best rationalization they can come up with.
Medicare is a single payer system that covers 1/6 of the nation and it works fine.
I don’t think it’s as impossible as you’re saying. It’s not like we’re talking about something brand new. Public health care is up and running all over the world. We can point to examples of how it’s working successfully in the real world. And there are precedents like Social Security and Medicare - the American people aren’t as opposed to big government services as they claim.
As for a specific path, I’m not ruling out Clinton. Keep in mind she got shot down over health care when she was First Lady. And she lost the 2008 election to Obama. I think she might carry a grudge. She might plan on getting a single-payer health care system enacted just to prove that she was right. She’d be saying “You could have had all this in 1993. You could have had this in 2009. But you wouldn’t listen to me.”
Medicaid is single-payer, and it does work, and it’s better than nothing.
I don’t think it’s “American exceptionalism” that’s stopping it. I think it’s a personal belief in one’s own exceptionalism. Not so much the average voter, but the average politician thinks he’s too exceptional to rely on government health care like some peon, and assumes his constituents, being brilliant high-achievers like himself, must feel the same way.
Also, there’s all that perfectly lovely money from the AMA.
One problem seldom talked about is that health insurers employ a ton of people. The overhead involved is very labor intensive. Single payer would reduce that overhead, leaving a small portion of the industry left for supplemental insurance. Many of those jobs are overseas, but a lot of them are in the U.S. The resizing of the labor force would likely be economically significant.
But I do think it would save lives. We were in London on the Tube and a guy was drunk. He managed to pass out to the point of being unresponsive. The British solution to this - a med team met him on the next platform, took him to the hospital, where they made sure he didn’t die of alcohol poisoning. I was with someone from there and I said we’d never do that in the U.S. She asked why. I said “you don’t saddle someone you don’t know with a hospital bill - they might not be insured.” I once provided first aid to a pedestrian hit by a car - she was obviously hurt - probably had broken bones, had trouble breathing, almost certainly had a concussion, likely in shock, but conscious. she refused an ambulance - a hospital trip would bankrupt her (and it was a hit and run, so she wasn’t getting the other guys insurance to pay). Now, it also costs money to get drunks to the hospital and pump their stomachs (or whatever they do) - but quicker treatment for injuries (and alcohol poisoning) would result in less long term economic impact - faster recovery, less time off work, less rehab.
There is no way to single payer from our current system. Governments in the US spend half of the money spent on healthcare to cover half the people, so in order for single payer to work government would have to double the money raised via taxation. However, the higher tax rates are the more deadweight loss occurs. So once you double everyone’s income tax you don’t double the money raised so you have to more than double everyone’s taxes. Because the US income tax system is so much more progressive than most of the rest of the world the burden falls on those who already have the highest rates. Because of this more than doubling the rates means you fall on the wrong side of the Laffer curve for many. So you have to really raise the rates for the poor and the middle class and even so it might still not be enough to raise sufficient revenue.
This is why every state that has flirted with single payer has backed off when they saw how much taxes would have to rise.
The only way to implement single payer is to go back in time and implement forty years ago.
The ironic thing is that Nixon almost created a single payer system paid for by payroll tax but Ted Kennedy refused the deal because the tax burden fell too much on the employee and not enough on the employer(LOL). FRK did do some good for his country.
Hmmm… this almost sounds like a suggestion that this should not be a federal government issue at all, and that it should be left to the states. Nah, that would make too much sense. Plus, it would might mean having to acknowledge the 10th amendment exists.
I’m not sure what the largest single payer nation is. Canada is physically large but only has 35 million people. Japan has a large population but not single payer.
What does this mean? If you saw an unresponsive person in the Metro you wouldn’t tell anyone? You wouldn’t call an ambulance?
Last summer, there were at least 3 times a homeless guy was laying unresponsive outside my work and someone called an ambulance, and twice they took the guy away to, I presume, a hospital.
If Premiums = Costs + Profits and Profits = (Premiums * x%), then when x (doesn’t it have to be less than 20% by law, now?) is constant and costs double, premiums also double, and therefore so do profits.
I’m not sure how much of that math is valid, but to this layman, it makes sense. It ignores the market’s value in setting prices, but the health insurance market is so not-free, I don’t even know how it responds to price fluctuations. It’s not like people can just find another health insurer when premiums go up, especially when the industry as a whole raises them the same amount.
Single payer can’t work in states because of Tiebout competition. If Vermont had gone through with single payer as they originally planned they would have had to jack up taxes so much, many people would have just moved to New Hampshire or Massachusetts. Most people can move much more easily to a new state then a new country so countries have much more leeway in how high their taxes can go in the short term.
{kind=link}